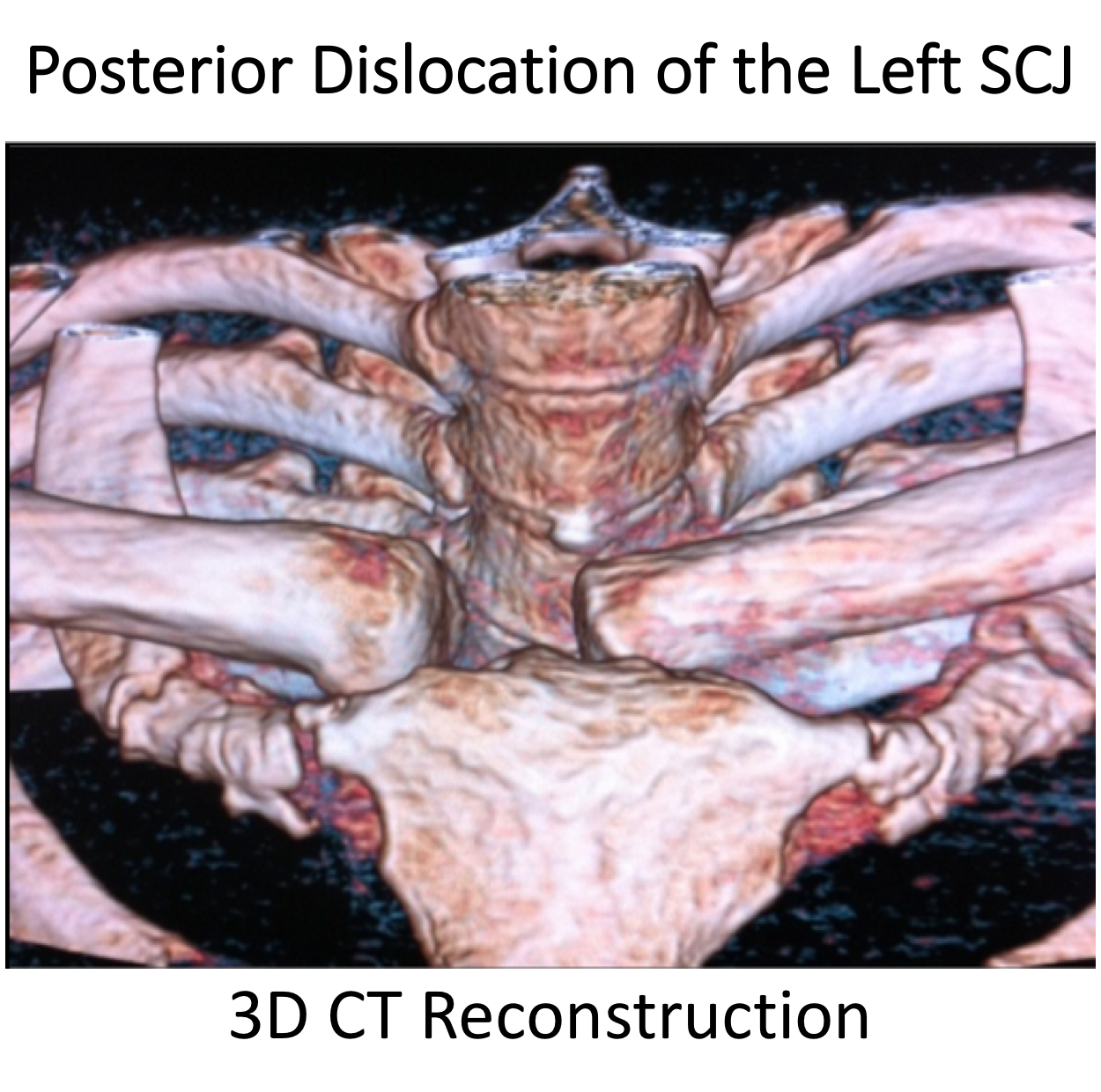
Posterior Dislocations
Posterior SCJ Dislocations
- Posterior Dislocations of the SCJ are rare
- Due to the close proximity of the large arteries and veins of the neck, which lie directly behind, Posterior Dislocations of the SCJ can be life threatening
- Dislocations can either be Traumatic, as the result of a significant injury, or Atraumatic, due to a combination of tissue laxity and muscle imbalance
SCJ Stabilising Structures
- The SCJ is held in joint by a combination of Static and Dynamic stabilising structures that work together to create an ‘envelope’ of stability
- Static Stabilisers - these are the capsular and ligamentous structures that surround the joint and include,
- Anterior & Posterior Sternoclavicular Ligaments
- Interclavicular Ligament
- Costoclavicular Ligaments
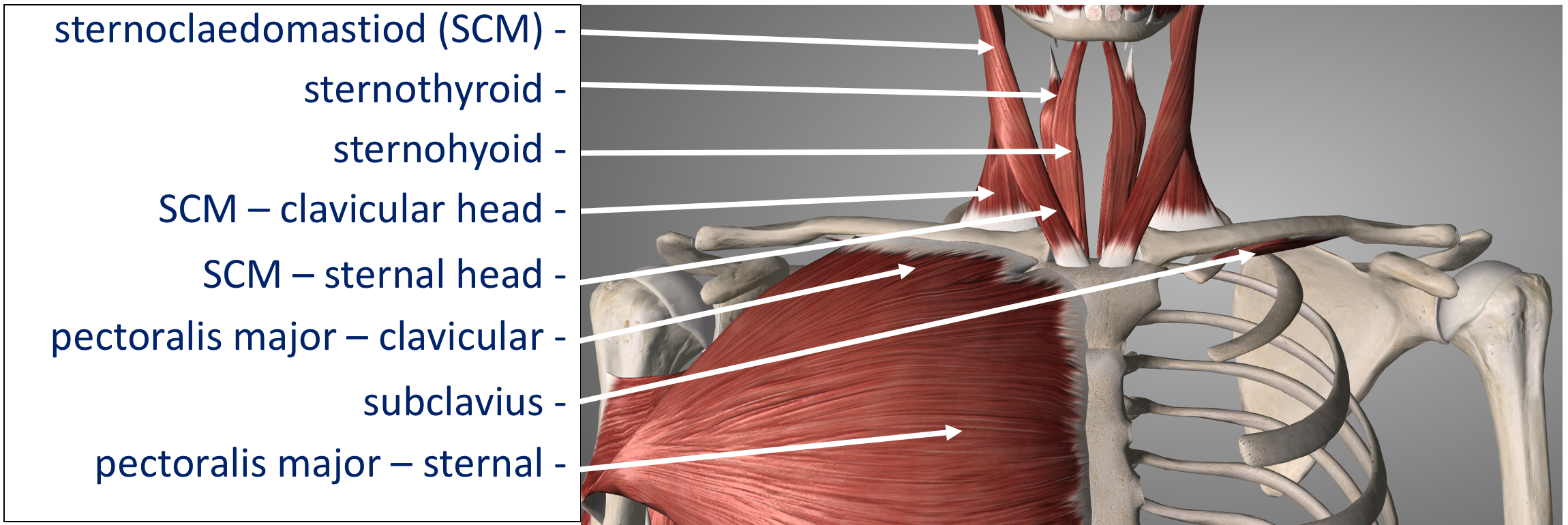
- Dynamic Stabilisers – the various muscles that attach to the clavicle and sternum all create a certain pull on the bones. The pull of these muscles is co-ordinated to precisely balance each other out, creating a ‘dynamic equilibrium, similar to guy ropes holding up a tent. Key muscles include,
- Subclavius
- Sternocleidomastoid (SCM)
- Pectoralis Major
- Static Stabilisers - these are the capsular and ligamentous structures that surround the joint and include,

What Happens? – Mechanism of Injury
- Traumatic SCJ Dislocation
- Traumatic SCJ Dislocations occur as the result of a significant injury that results in the sternoclavicular, interclavicular and costoclavicular ligaments being torn and the medial end of the clavicle being forced backwards
- The mechanism of injury is usually due to an indirect, oblique force aimed forwards on to the outer end of the back of the shoulder
- This force causes shoulder and lateral end of the clavicle forwards whilst rotating the medial backwards, away from the sternum, rupturing the ligaments
- Less commonly, a direct force from the front onto the medial end of the clavicle can rupture the SCJ ligaments, dislocating the clavicle backwards


- Atraumatic SCJ Dislocation
- Atraumatic SCJ Dislocations tend to occur in younger patients under the age of 20 years
- Sometimes there is a relatively minor indirect force that precipitates the initial dislocation but, usually, the SCJ spontaneously begins to dislocate without an injury
- The medial end of the clavicle dislocates due to a combination of increased laxity in the stabilising ligaments and an abnormality in the sequence in which the envelope of stabilising muscles work
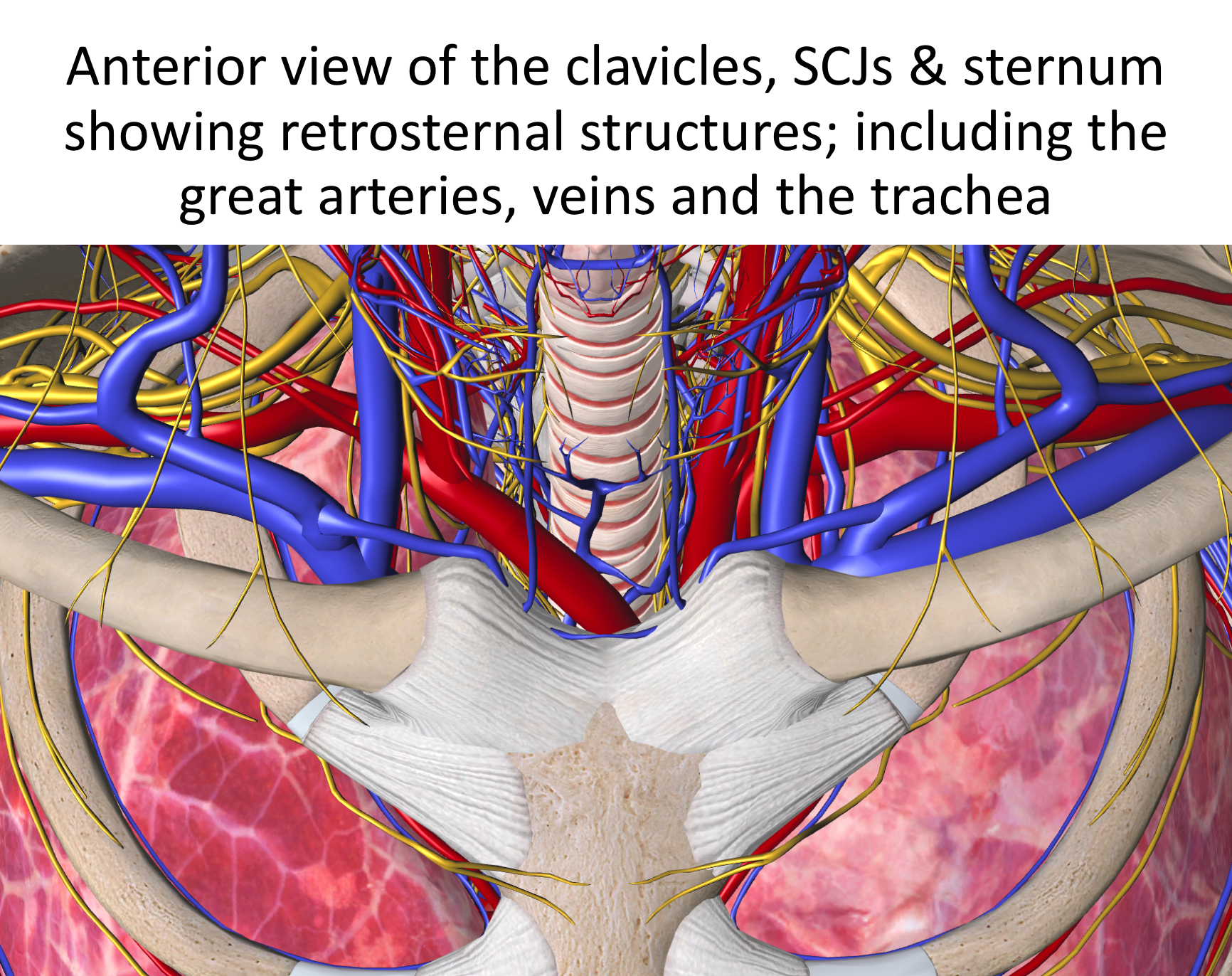
Why is a Posterior SCJ Dislocation so Dangerous?
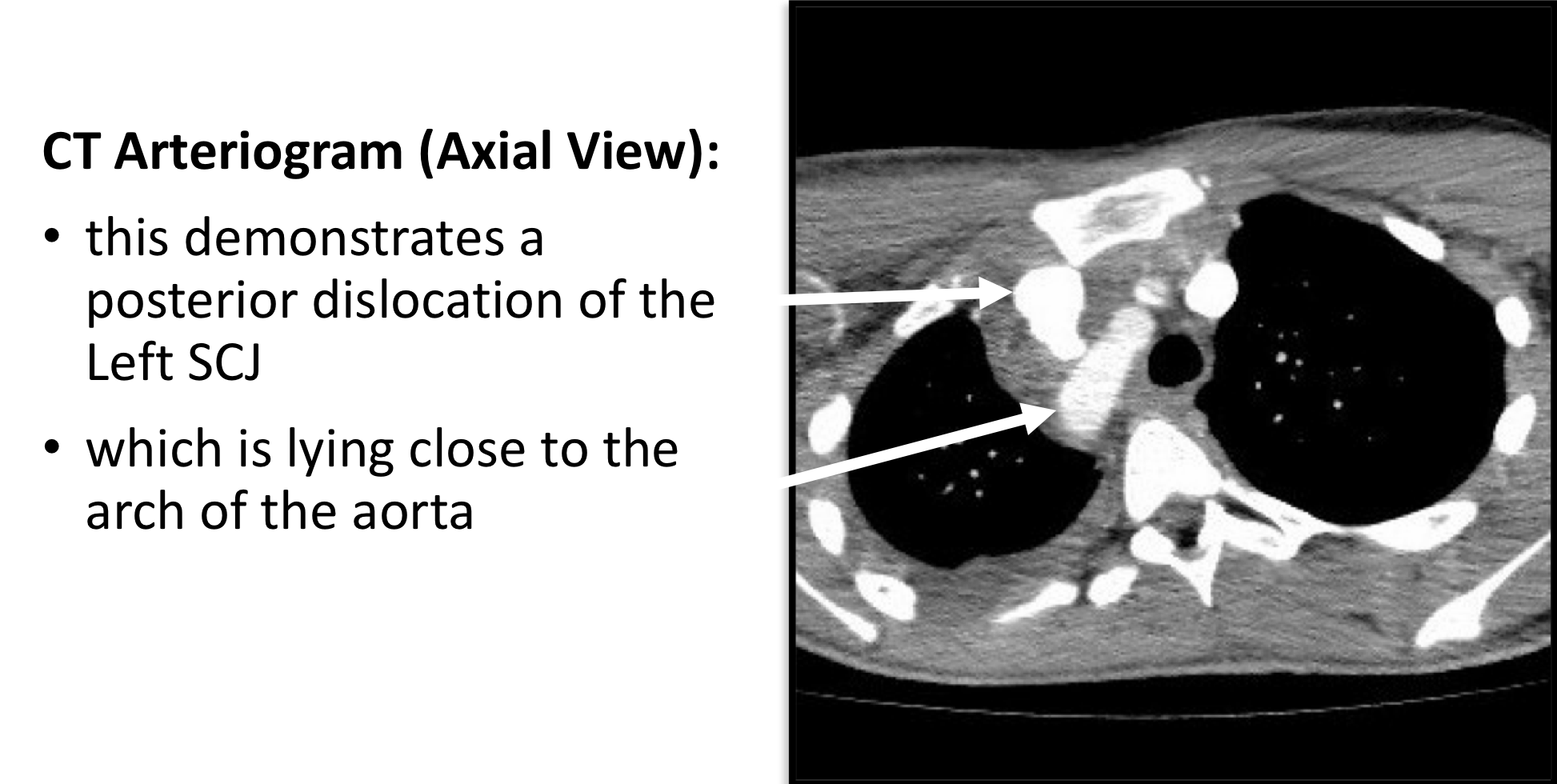
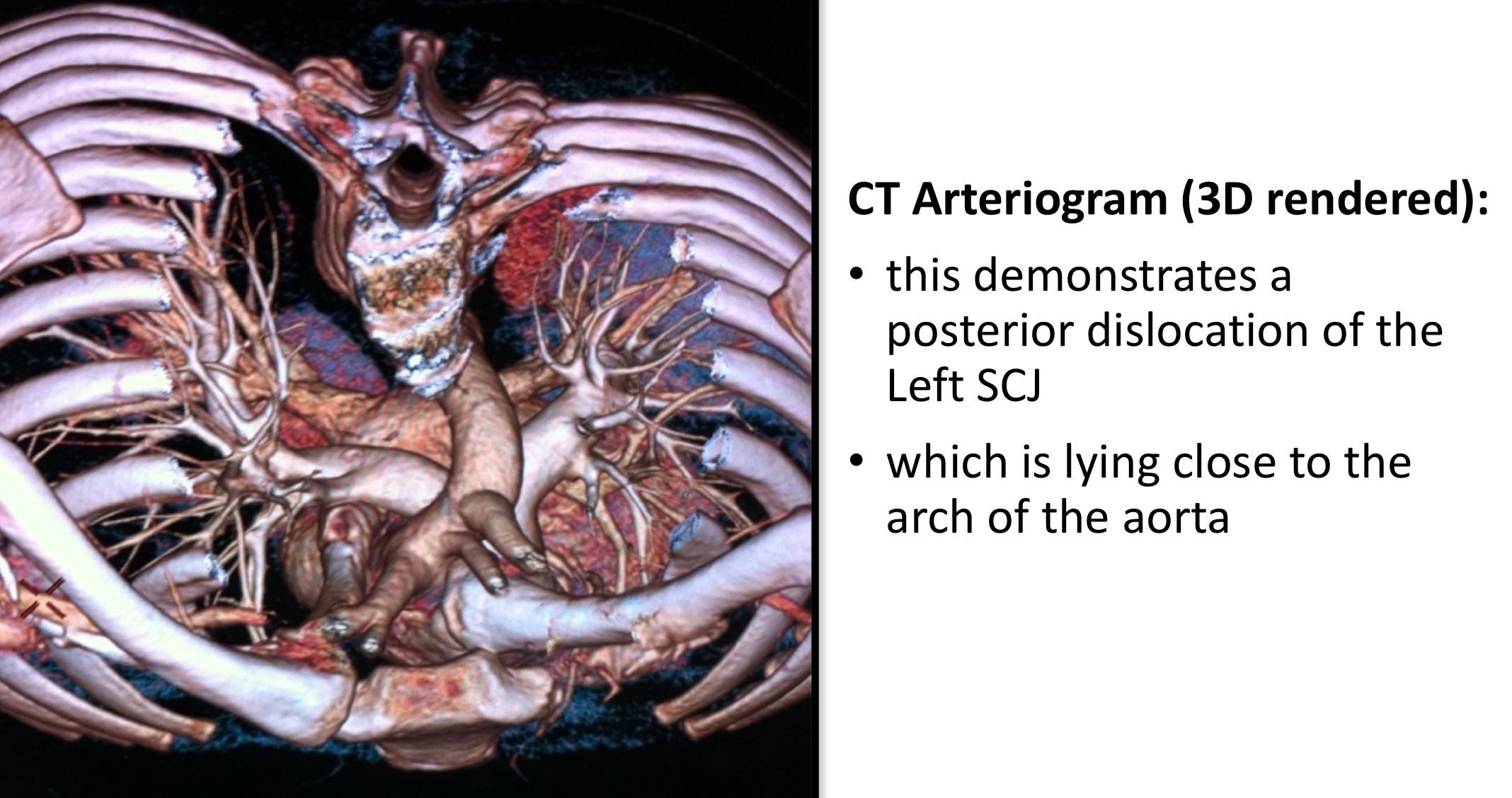
- The Arch of the Aorta and the Great Vessels and Veins, which supply the head and neck, lie directly behind the sternum and the SCJs
- The larynx of the throat and the pharynx of the oesophagus lie directly behind these structures
- Collectively, these are known as the Mediastinal or Retrosternal structures
- When the medial end of the clavicle is dislocated backwards, during a posterior dislocation, all of these structures are potentially vulnerable to injury
- At the time of an Acute dislocation injury and rupture to one of the great vessels or veins could lead to a catastrophic haemorrhage
- If the medial end of the clavicle remains dislocated, in a Chronic dislocation, it can put pressure onto an artery, vein or the larynx and pharynx potentially leading to erosion of these structures

How do you Diagnose a Posterior Dislocation?
As with any condition assessment begins with a history and examination of the patient. These can be very different following an ACUTE injury when compared to a CHRONIC problem
- History - ACUTE
- The force required to sustain an Acute Posterior SCJ Dislocation is usually very significant and it is important to get as much information about the mechanism of injury
- Initially it is most important to assess for any symptoms of Mediastinal compromise; these would include – difficulty breathing or swallowing, severe retrosternal pain and a feeling of faintness or swelling around the neck
- RECENT / CHRONIC
- Patients may have noticed that the SCJ feels abnormal where the clavicle has dislocated posteriorly. This can sometimes lead to the whole shoulder girdle ‘protracting’ forwards resulting in the scapula sticking out, which can be painful on shoulder movements and when sitting backwards

- Examination –
- Following an ACUTE injury it is essential to assess the patients cardiovascular and respiratory function looking for any compromise
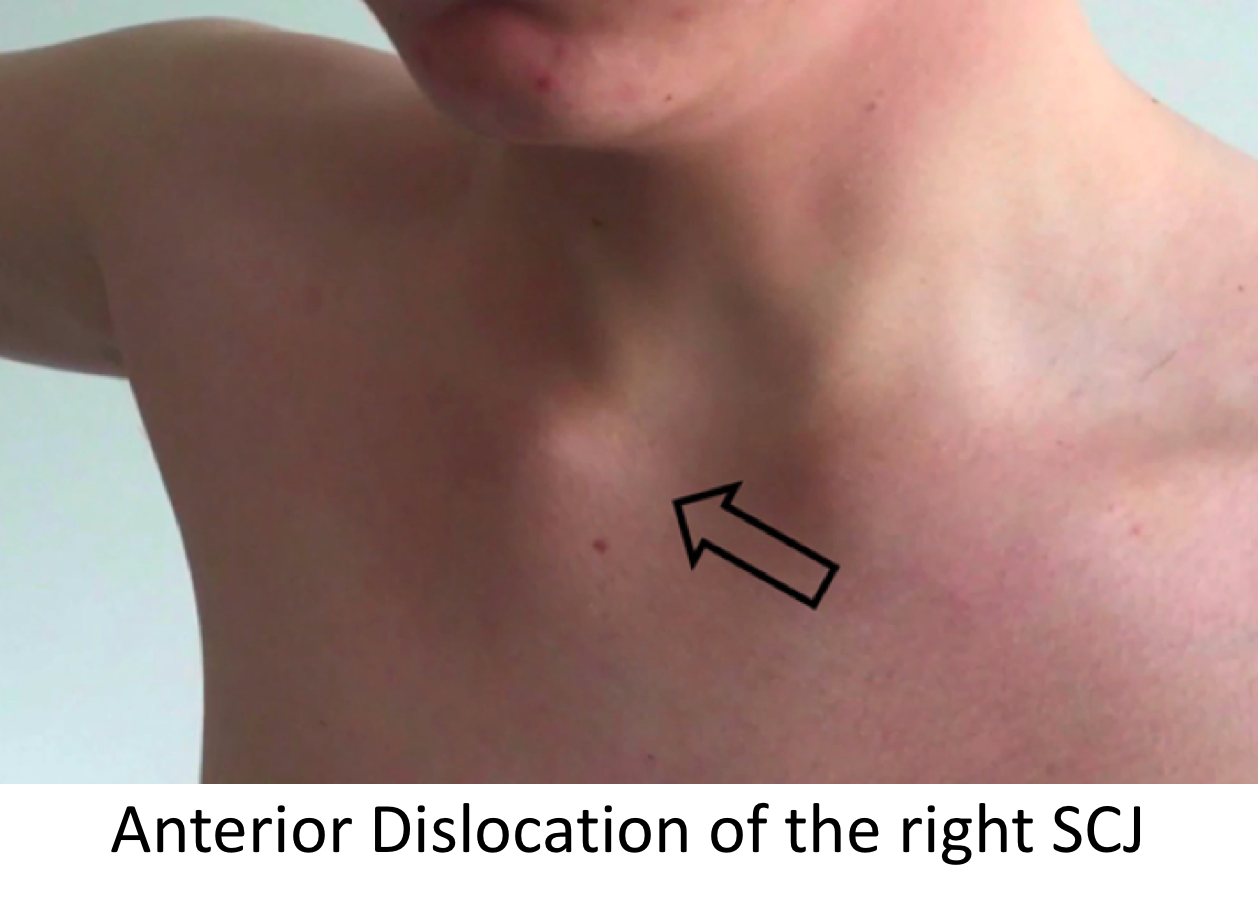
- The contour of the clavicle is usually abnormal with the medial end displaced backwards, when compared to the un-injured side
- The whole of the shoulder girdle may be protracted forwards and the scapula winged. This may lead to abnormality of the glenohumeral function

- Investigations –
- CT & CT Arteriogram – due to the potential compromise or damage to the mediastinal structures lying directly behind the SCJ I would consider a CT to be an essential base-line investigation. Following an acute injury and if surgical stabilisation is going to be considered for recurrent instability a CT arteriogram should be undertaken
Management of Posterior SCJ Dislocations / Instability
The initial management of an ACUTE Posterior SCJ dislocation differs from a RECURRENT/CHRONIC dislocation. In the acute situation it is essential to treat the patient for any associated mediastinal injuries. These can be obvious at the time and involve active bleeding or my involve the clavicle having penetrated a vascular structure which may be compromised at a later date.
In the case of an acute Posterior Dislocation my recommended treatment is to undertake and open reduction and a Figure-Of-Eight Autograft Hamstring Tendon Reconstruction. In certain cases, particularly in younger patients, where their soft-tissues are very good, the joint can be stabilised by repairing the soft-tissue structures and augmenting this with an Internal Brace implant. Whilst closed reductions have been recommended, my concern, is that in doing this, there may be damage to the retrosternal structures, which is not initially noticed, and there is also a very high re-dislocation rate.
For a patient with symptomatic recurrent dislocations or a chronically dislocated SCJ my treatment of choice is, again, a Figure-Of-Eight Autograft Hamstring Tendon Reconstruction.

Surgery for Posterior SCJ Dislocations / Instability
For an Acute or Chronically dislocated SCJan Anterior SCJ Reconstruction using a Figure-of-Eight Hamstring Tendon Autograft is my procedure of choice., I undertake these procedures in combination with my Thoracic Surgery colleagues. The procedure is undertaken under a General Anaesthetic and usually requires an overnight stay.
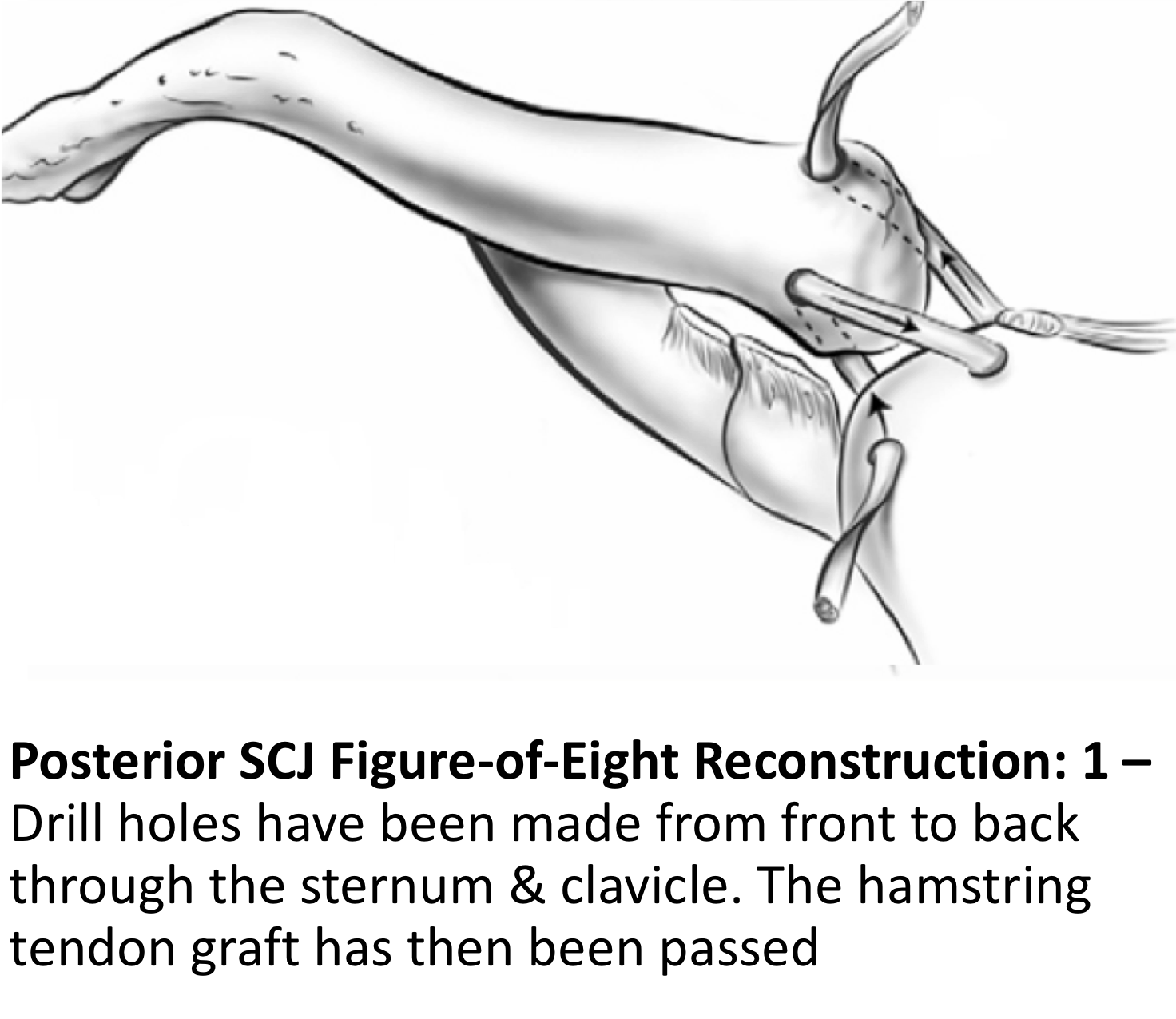
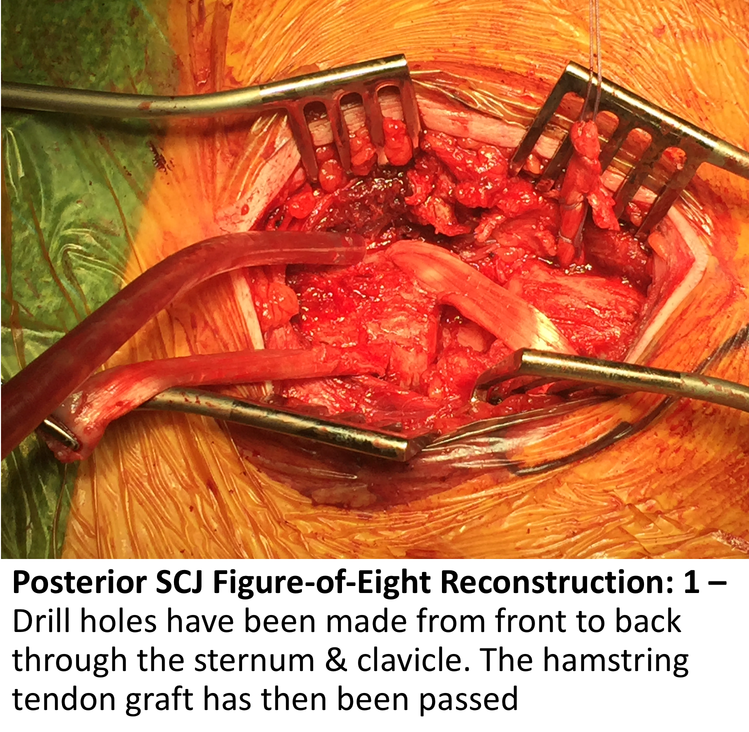
The whole of the patient’s chest is prepared so that, in the unlikely case, a midline sternotomy can be undertaken. Using an oblique incision over the SCJ the medial end of the clavicle and the lateral side of the sternum are exposed. Whilst protecting the retrosternal structures two, 3.5mm drill holes are made through each bone from front-to-back. The Gracilis hamstring tendon is then harvested from the patients knee and prepared. The tendon is then passed through the drill holes in the bones in a figure-of-eight fashion, tightened and sutured into position. The repair is then protected with an Internal Brace. In certain situations, where a patient has previously had a hamstring tendon graft for another procedure or where there might be concerns with regards to the suitability of the patient’s own tendons, a donor allograft hamstring tendon may be used.
My routine Anterior SCJ Reconstruction is described below,
- The patient is anaesthetised with a general anaesthetic and prophylactic antibiotics are given
- A 10 cm incision is made over the SCJ and the damaged and the medial end of the clavicle and lateral end of the sternum exposed
- Dissection is taken posteriorly, protecting the retrosternal structures
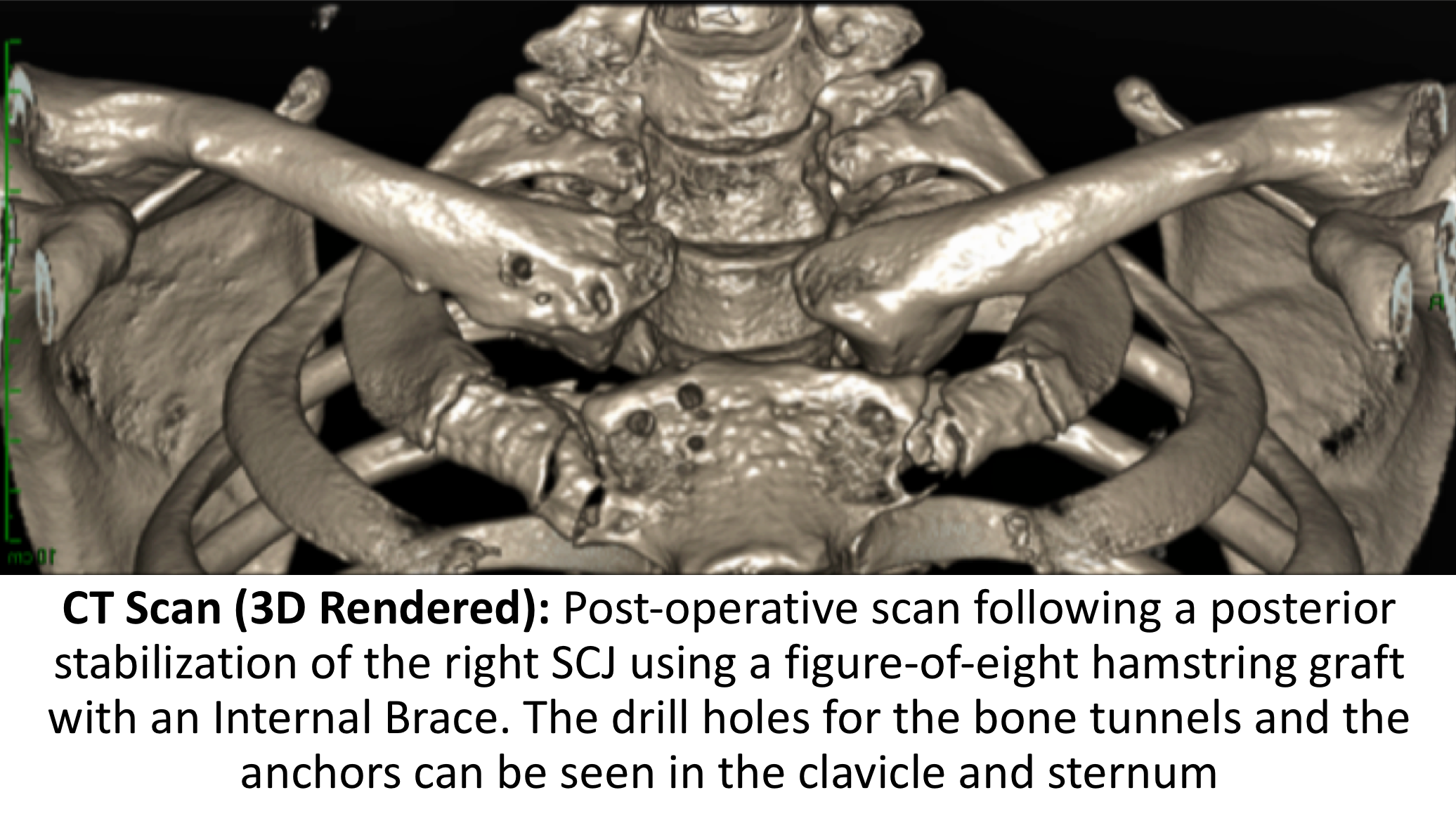
- Guide wires are carefully drilled through the bones from front-to-back and then overdrilled with a 3.5cm drill to create 2 drill holes in each bone
- Through a 5cm incision, just below the knee, the Gracilis hamstring tendon is harvested and prepared with a full length FibreWire whip stitch
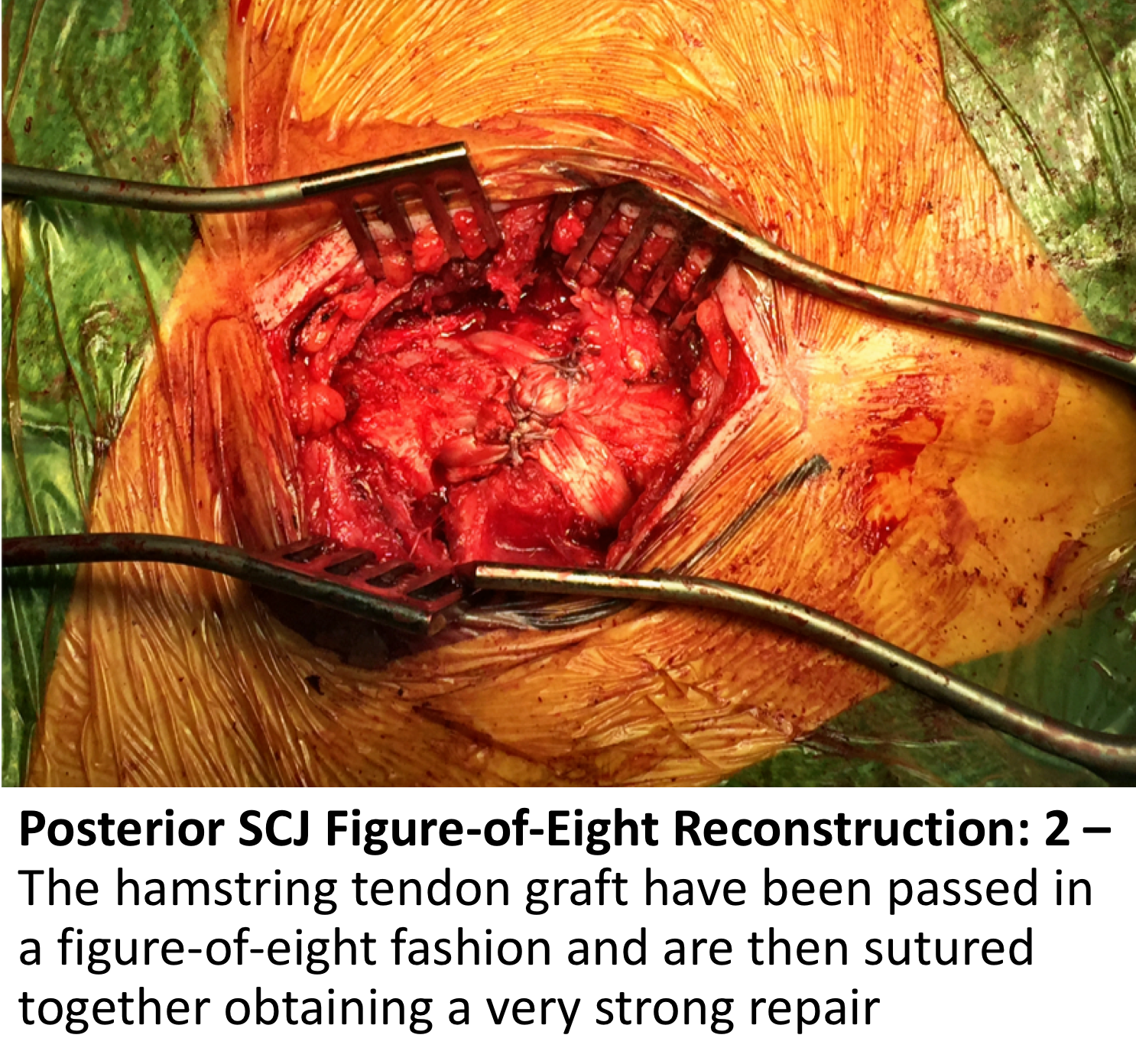
- The prepared tendon is then passed between the drill holes in the clavicle and sternum in a figure-of-eight fashion
- The tendon is then tightened and its ends securely sutured in position
- Using an Internal Brace system, Biocomposite Swivelok Anchors are then inserted into each bone with a double FibreTape tightened between them
- The repair is then inspected, washed out and the wound closed in layers
- Local Anaesthetic is then infiltrated around the wound

After the Surgery
Post-Operative Care
Following an Anterior SCJ Reconstruction the patient will usually stay in the hospital overnight.Either a CT Scan or Digital Tomogram will be taken the next morning to assess the repair. I would see the patient after the surgery to discuss how the procedure has gone and arrange for further Follow-Up. The patient will be seen by the In-Patient Physiotherapy team, who will instruct them on the initial Rehabilitation Protocol for their shoulder. Further Out-Patient physiotherapy will then be organised.
I would usually review patients in the clinic 1 month and 3 months after their procedure to assess their progress and recovery.
Rehabilitation Protocol
Immediately after the surgery, when the patient has woken up from their general anaesthetic, the SCJ is numb from the local anaesthetic. The SCJ may be painful once the local anaesthetic has worn off which is usually adequately controlled with routine oral analgesics which will be prescribed. I encourage patients to get their arm moving as quickly as possible, discomfort permitting.
After an Anterior SCJ Reconstruction, it is initially important to ‘protect’ the repair from any significant load, and patients should restrict their arm movements to below shoulder height. Patients would usually need to have their arm in a broad-arm sling for 4 weeks and use their arm when in a safe environment.
My standard rehabilitation protocol is outlined below. The information and time to recovery are a general estimation and may vary from person to person.

|
Post op |
|
| Immediate |
|
|
Day 1-4 Weeks |
|
| 4-8 Weeks |
|
|
Milestones |
|
|
Week 4 |
Full passive range of movement |
|
Week 8 |
Full active range of movement, good scapular control |
|
Return to Functional Activities |
|
| Driving |
|
| Swimming |
|
| Golf |
|
| Racquet Sports/Repeated Overhead Activities |
|
| Lifting |
|
| Work |
|
Success of Surgery, Risks & Complications
An Anterior SCJ Reconstruction is usually a very successful procedure but, because it takes some time for the reconstructed tissues around the SCJ to recover, it usually takes between 6 months for the SCJ to be as good as it can be.
There are always risks and complications associated with any operation.
- Anaesthetic - The risks of having a General Anaesthetic are very low, but will always need to be assessed on an individual basis by an Anaesthetist. Suffice it to say, that whilst a Shoulder Operation can in no way be considered a ‘life-saving’ procedure, an Anaesthetist would not consider undertaking an anaesthetic if they had any concerns that an undue risk was being taken.
- Infection – Infection following arthroscopic surgery is rare < 0.2%
- Neurovascular Injury – Damage tosignificant neurovascular structures during open Anterior SCJ surgery is rare, but can be catastrophic < 1%
CRPS Type 1 – A Chronic Pain Syndrome following arthroscopic shoulder surgery is rare < 0.2%
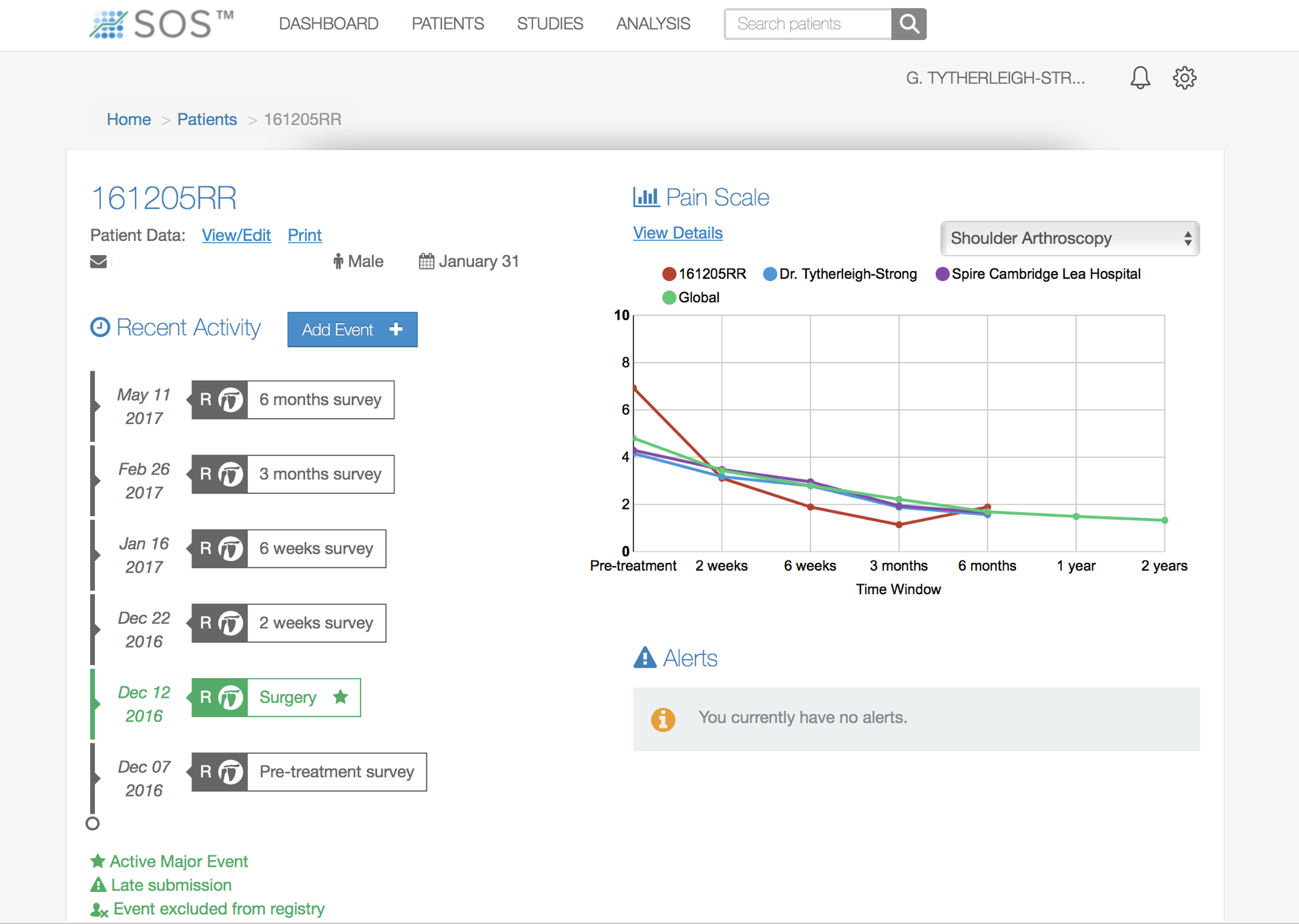
Outcome Measures
Assessing patient outcomes following surgery, using validated scoring systems, is a very important and useful exercise.
find out more about the SOS outcome system…