








Rotator Cuff Tears
Rotator Cuff Tears (Torn Tendon)
-
Everyones’ Rotator Cuff Tendons undergo ‘wear and tear’ over time. This can lead initially to a Tendonitis and then, as the tendons become weakened and thinned out, to Partial or Complete tears.
-
This process is often going on quietly in the background and many people, over time, develop tears without any symptoms and without knowing about it. In an MRI scan study of people over 60 who felt that they had no problems with their shoulder, over 40% had a tear of some size of their Rotator Cuff on their scans!
-
However, some people with a Rotator Cuff Tears do develop symptoms. These maybe sparked off by a specific incident or accident, where an acute tear occurs in an already weakened or previously torn tendon. In other people the symptoms may develop slowly representing the progression of a Supraspinatus Tendonitis.
-
Regardless of the way that the symptoms of a Rotator Cuff Tear start, when they do occur they usually require some form of treatment to settle it down.
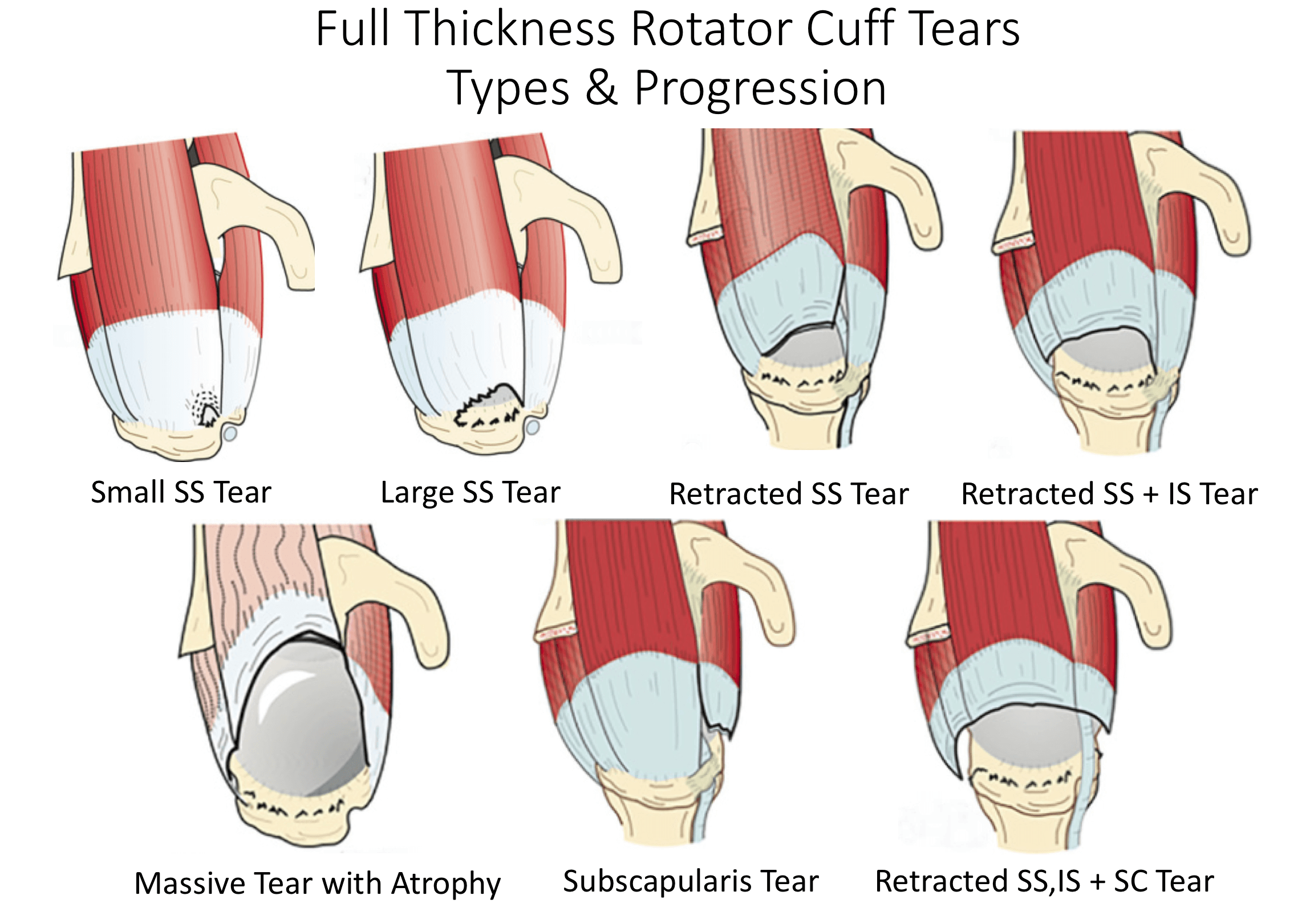
Types of Rotator Cuff Tears
There are many different types of Rotator Cuff Tears and different ways that they can be classified. I prefer to look at Tears in the way that they can be treated. I categorise them as either being Acute or Chronic, which Tendons have been Torn, whether they are Partial or Full Thickness Tears, how big they are and whether it will be technically possible to repair them. Other considerations are the quality of the tissue and fatty atrophy, other associated shoulder problems and the age, health and expectations of the individual patient.
-
Acute v Chronic Tears – most Rotator Cuff tears are chronic and have slowly developed over time. However, sometimes patients can sustain an acute or an acute-on-chronic tear following a specific injury or event. If in Acute Tear is repaired within 3 – 4 months of its onset, it is likely that it will heal better than if the repaired later. For chronic tears this time window is less important.
-
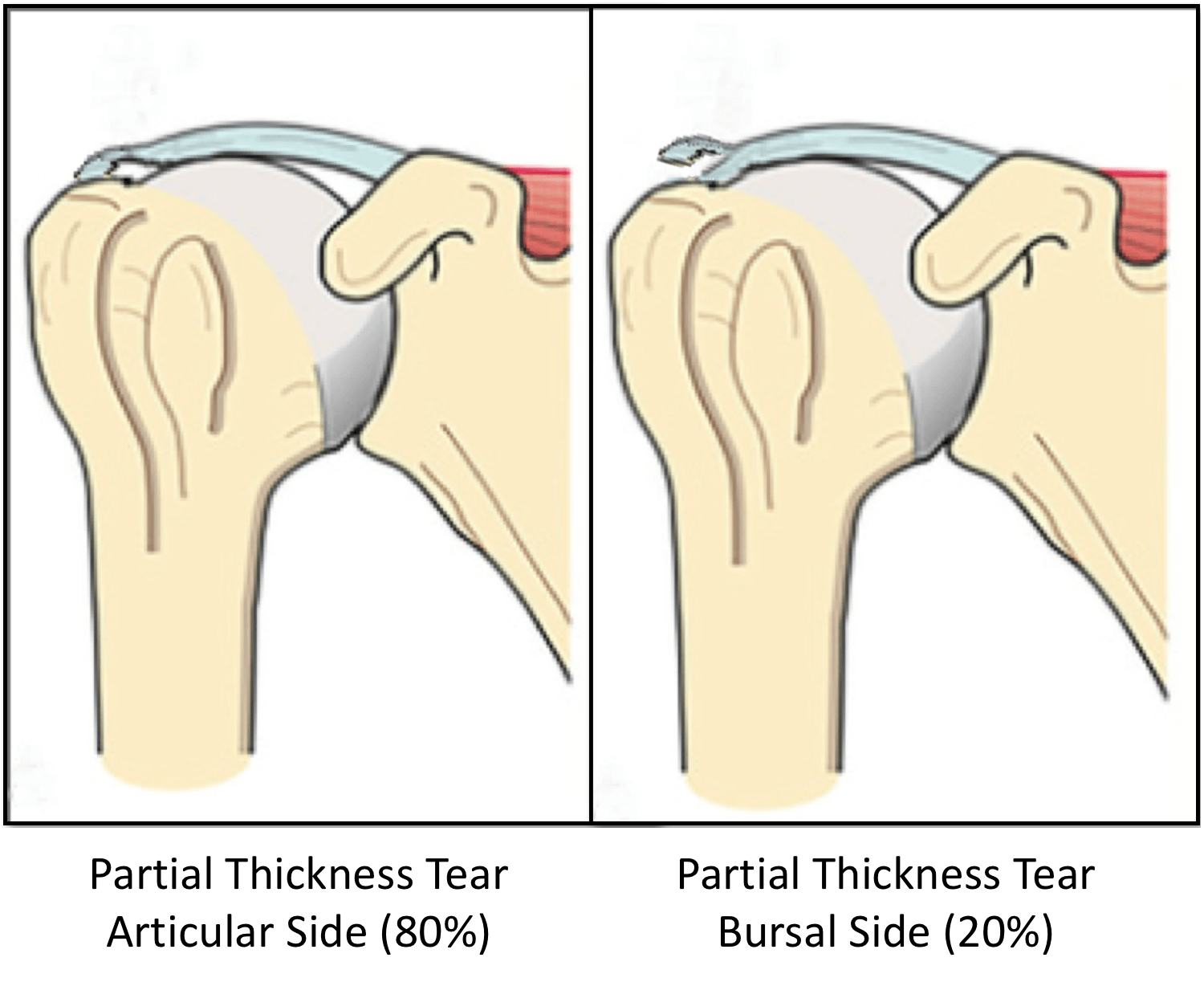
Partial v Full Thickness Tears –Partial Thickness Tears tend to occur in younger patients and at an earlier stage of Rotator Cuff Disease.
80% occur on the articular side of the tendon, which is thought to be the result of a ‘watershed’ in the blood supply to the tendon
Not all Partial Thickness Tears need to be repaired as they can sometimes heal or may not progress.
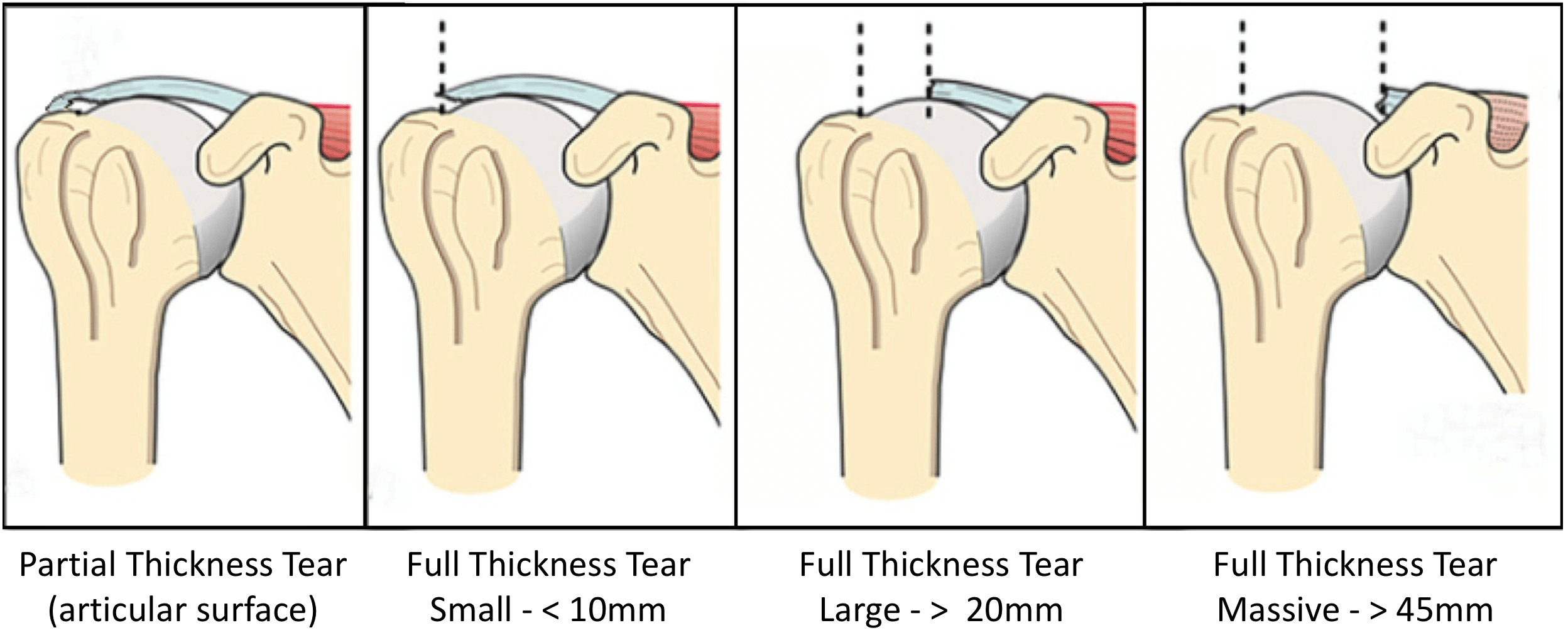
However, as a general rule, the bigger the size of the tear, the younger the age of the patient and the more severe the symptoms are indications to surgically repair the Tendon as the tear is likely to progress over time.
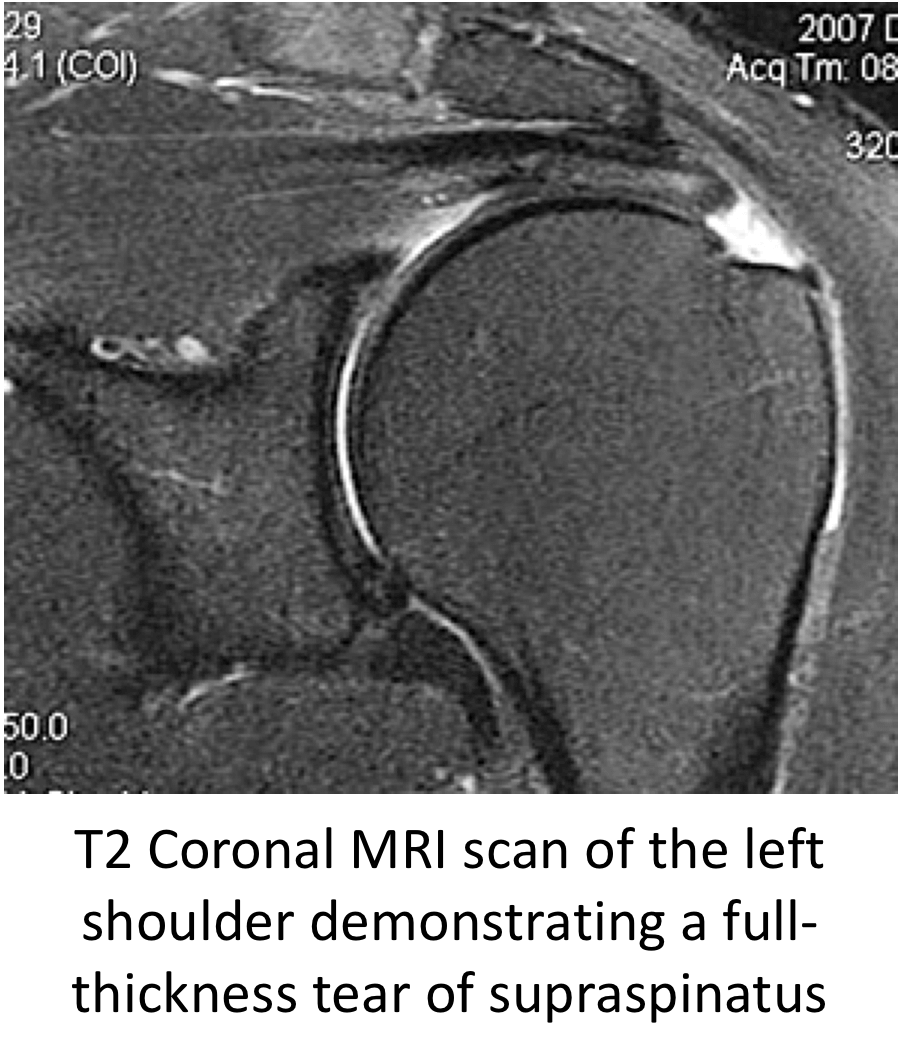
Full Thickness tears generally will NOT heal and probably, over time, will propagate further. Most symptomatic Full Thickness Tears will usually require a repair to settle the symptoms.
-
Size of the Tear – Rotator cuff tears tend to propagate over time.
- Tear size tends to be measured with regards to the distance with which the torn tendon has retracted from its insertion on the greater tuberosity.
- With advances in surgical technique and equipment it is now possible to repair even very large tears. However, there are still some situations where the tear is so massive, the tendon has begun to disappear or is so stuck and retracted that it may not be technically possible to undertake a repair.
-
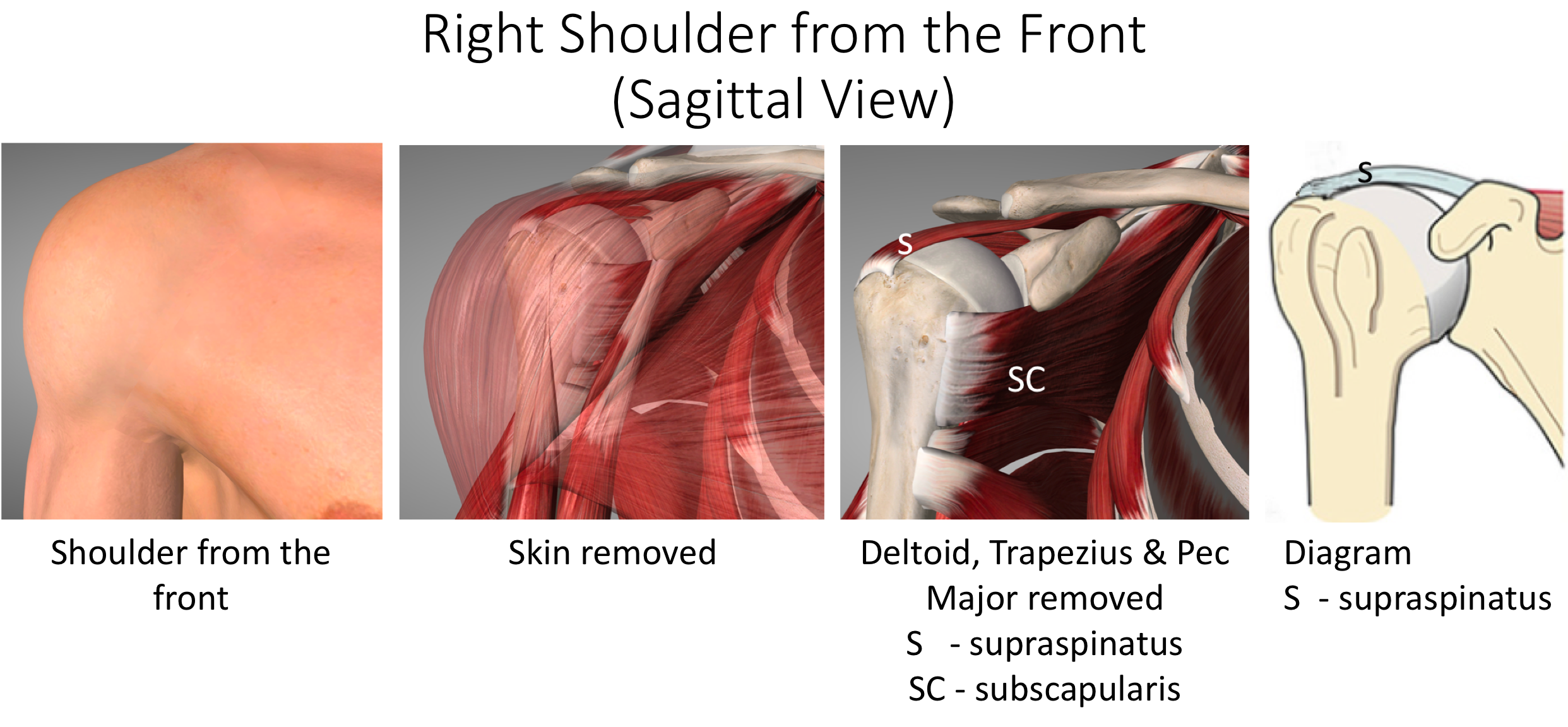
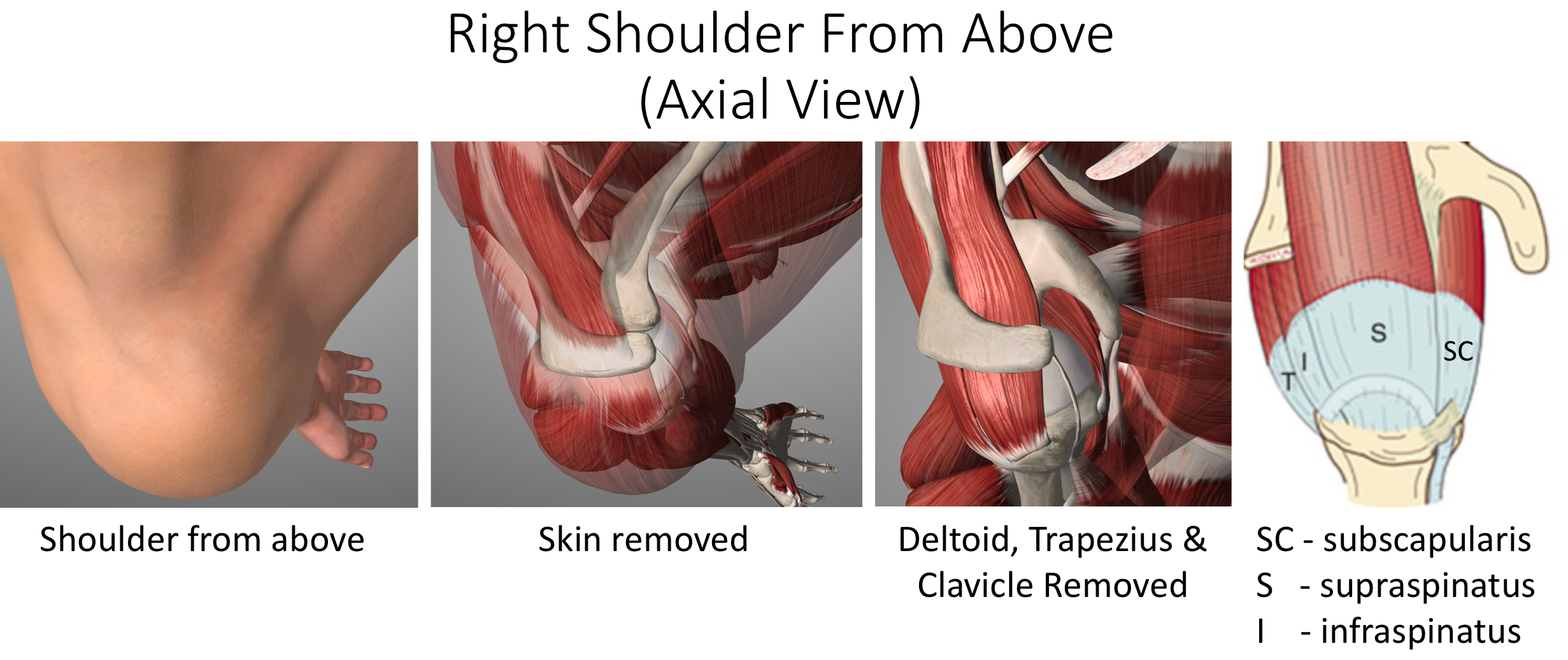
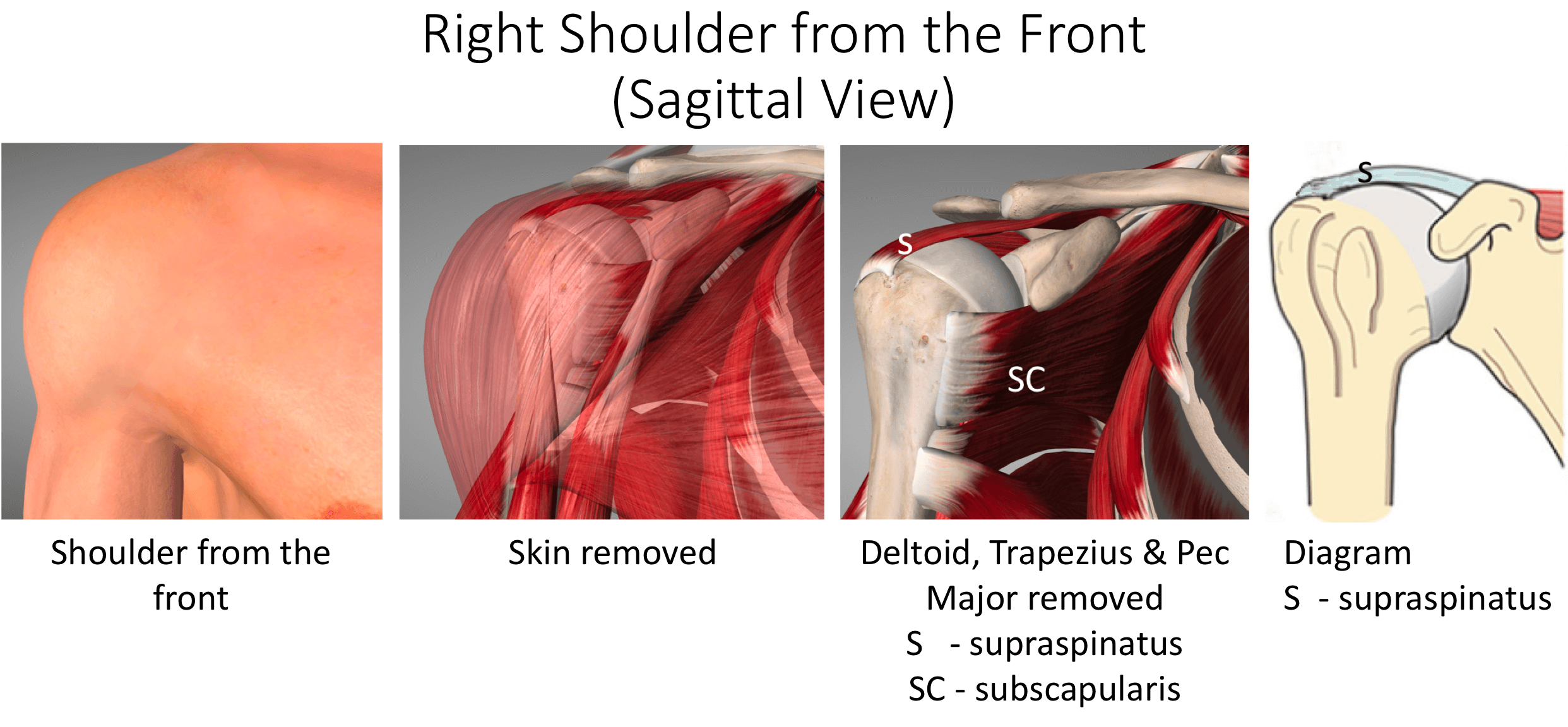
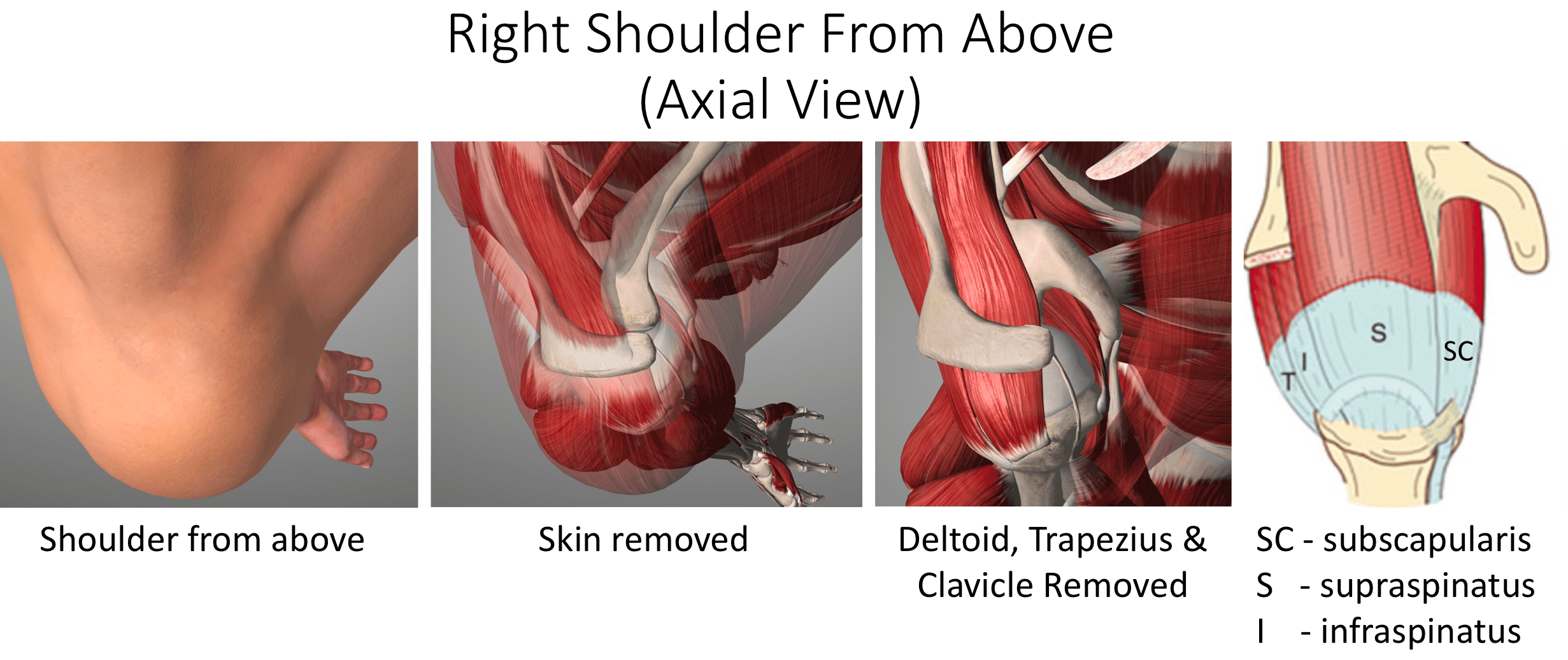
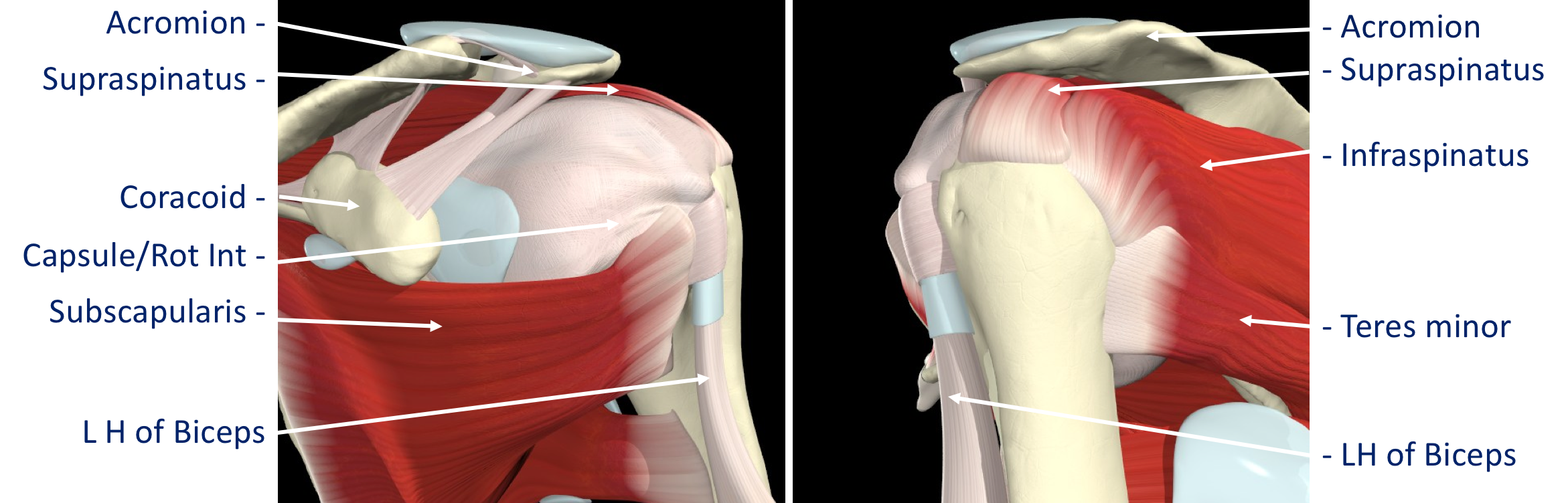
Which Tendon is Torn? – Although the Supraspinatus Tendon is the most commonly torn tendon, Infraspinatus and Subscapularis tears can also occur. Sometimes more than one tendon may be torn at the same time. The best way to treat specific tendons and combination tears can differ depending on the tendons involved.
-
Quality of the Torn Tendon – Rotator Cuff Tears usually occur in degenerate tendons. Sometimes the degeneration / wear and tear is so advanced that the actual quality of the torn Tendon is not mechanically strong enough to hold a repair and probably will not heal.
-
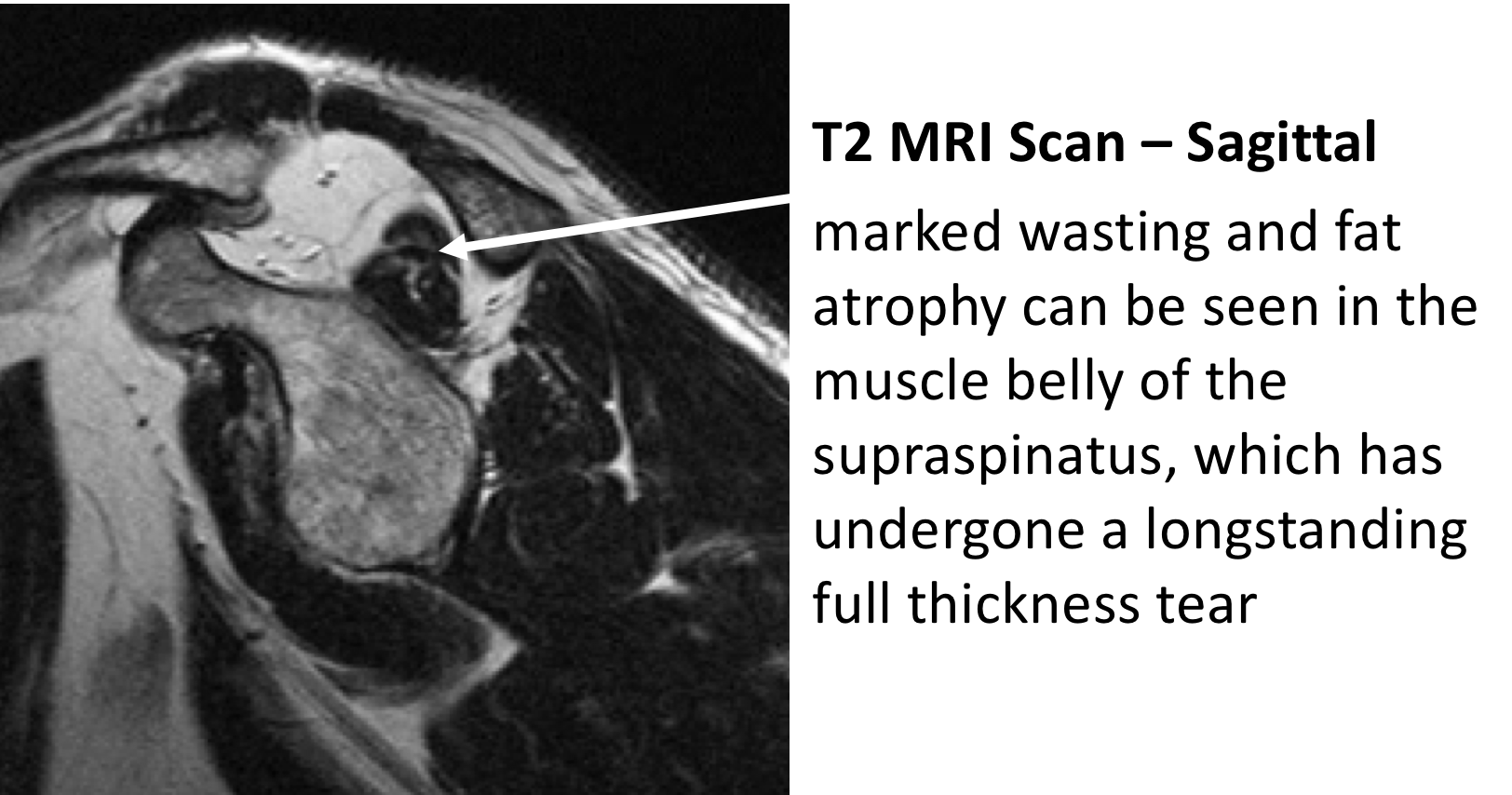
Fatty Atrophy -When a Tendon is torn, the muscle that it was connecting to the bone will no longer be able to work and undergoes Disuse Atrophy. If this situation is sustained the muscle cells may then begin to be replaced by fat cells, Fatty Atrophy. Unfortunately, this is an irreversible process and, even if the Tendon is repaired and the muscle re-activated, the muscle cells cannot be restored. If the muscle of a torn tendon has undergone significant Fatty Atrophy, even if the tendon can be technically repaired, it will not regain its function.
-
Associated Shoulder Problems –Rotator Cuff Tears are often associated with other wear and tear problems in the shoulder. These include Long Head of Biceps Tendonitis, AC Joint problems and Shoulder Joint Osteoarthritis. How significant the Rotator Cuff Tear’s contribution is to a patient’s symptoms, when any of these associated problems are present, may determine how it is best treated.
-
Age, Health and Patient’s Expectations – I look at age Physiologically rather than Chronologically!! Younger patients usually have a better healing potential, are more active and will have higher functional expectations. As a result, they are likely to heal better and more quickly following a bigger procedure and may be more tolerant of undergoing a protracted recovery period to gain the best function possible. Older patients and patients with other significant health issues may not heal as well and are only looking for pain relief and a recovery of normal day to day function. They may be less prepared to undergo a ‘heroic’ procedure with a protracted recovery to gain the best function and would prefer a less complex procedure with a quicker recovery of acceptable function.
What are the Symptoms of a Rotator Cuff Tear?
-
As with a Supraspinatus Tendonitis ‘wear and tear’ plays a considerable part in the development of Rotator Cuff Tears and the onset of symptoms can often be quite insidious. As a result, many people find that their symptoms gradually develop over time. In other cases, a specific injury or incident can create a tear or propagate further a chronic tear and spark off a sudden onset of symptoms.
-
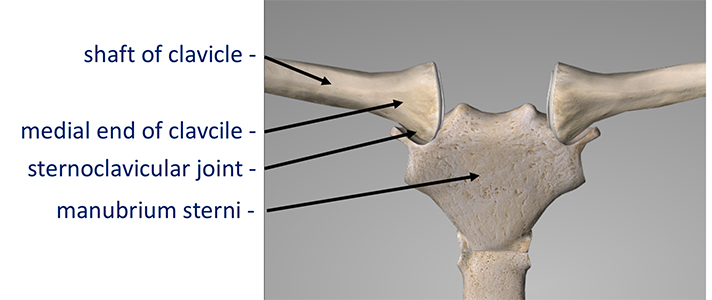
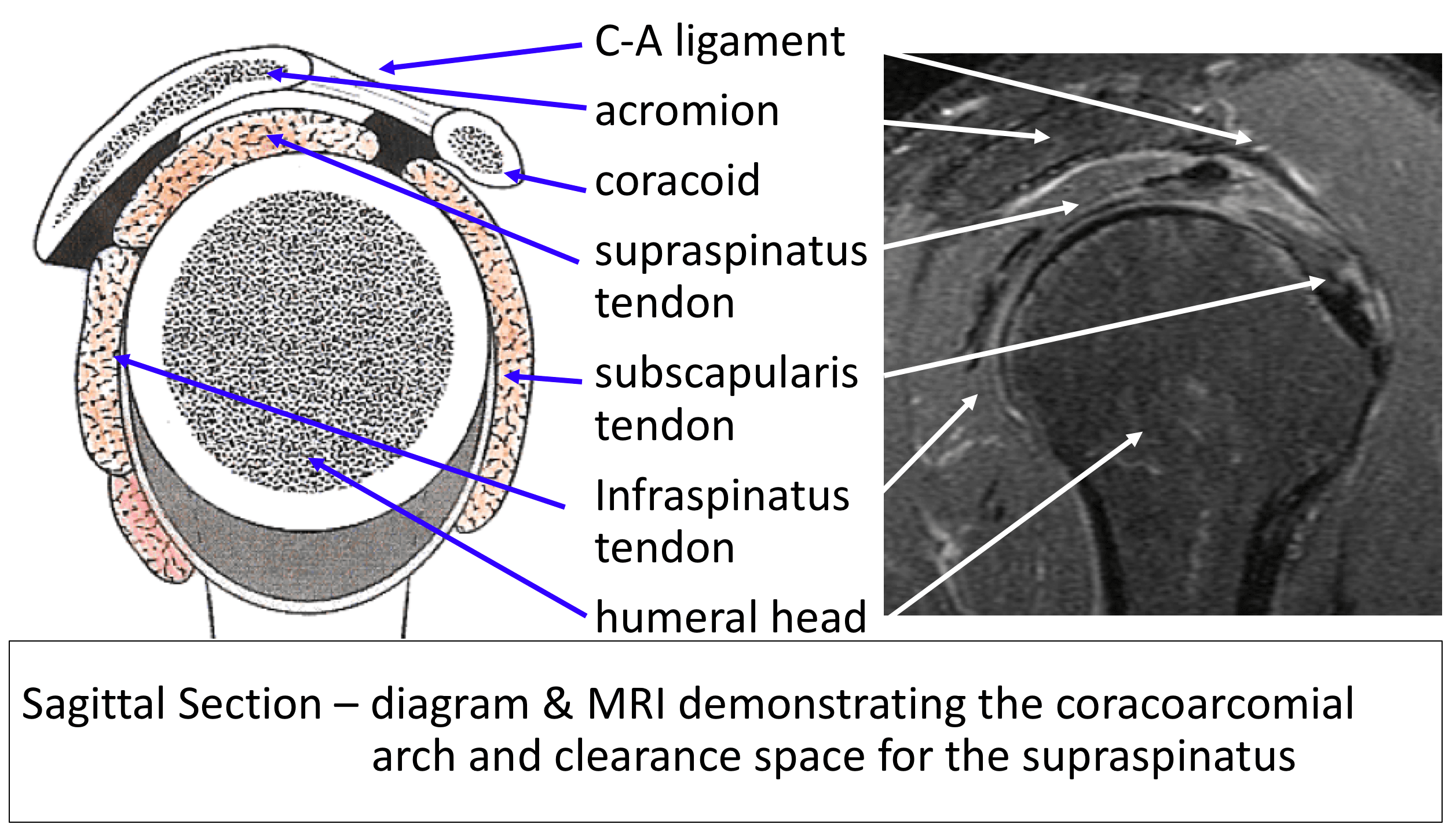
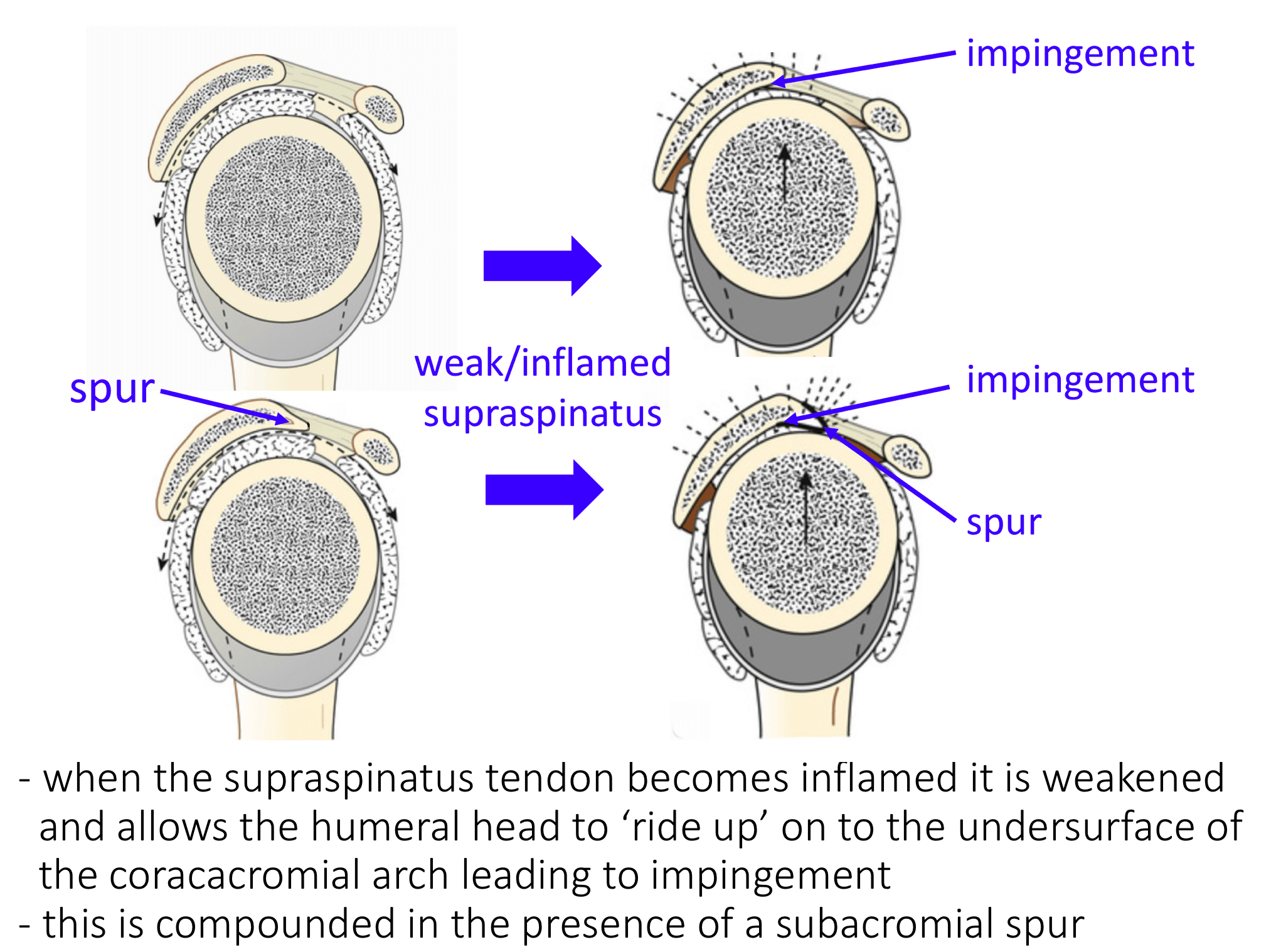
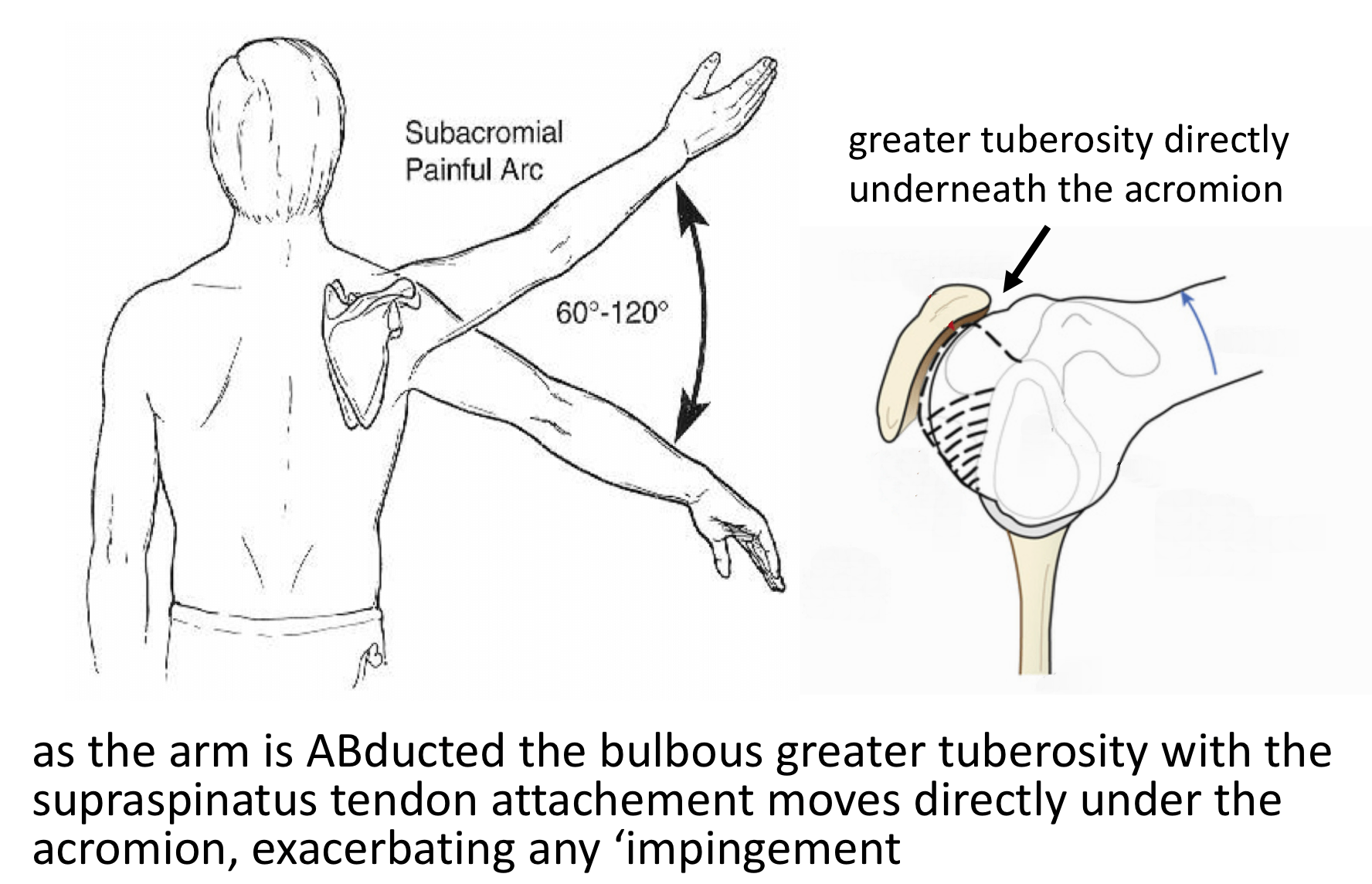
There is a bulge on the side of the Humeral Head (Greater Tuberosity) where the Supraspinatus and Infraspinatus Tendons insert into the bone. As the shoulder moves, this bulge lies directly under the acromion between 60 and 120 degrees of elevation. This is the point where the space between the top of the Humeral Head and the Acromion is the narrowest. This is known as the ‘Painful Arc’ of movement..
-
The early symptoms of a Rotator Cuff Tear tend to be a background pain over the shoulder with particular discomfort when elevating the shoulder within the ‘Painful Arc’ and associated weakness. The shoulder is often uncomfortable to lie on at night.
-
As symptoms deteriorate the shoulder becomes increasingly painful all of the time. Pain tends to occur on more directions of movement and the shoulder can appear to become weaker. Night discomfort often becomes more of a feature.
-
With chronic shoulder pain, the muscles that help to stabilize the scapula often try to hold the shoulder up, in a more protected position. Overtime these muscles can begin to ache so that the pain can appear to radiate up towards the neck and over the shoulder blade.
How do you Diagnose a Rotator Cuff Tear?
-
History – Most people notice a gradual onset of pain and discomfort over the top and side of their shoulder. Sometimes people can identify a specific injury or incident that triggered their problem. They may notice particular pain on elevating their arm and in bed at night. As the condition deteriorates they may get pain more of the time and on more directions of movement. They also might notice some weakness. In extreme cases they may not be able to actively elevate their shoulder at all
-
Examination – Occasionally the patient can experience some discomfort on palpation over the front edge of their Acromion. In the case of longstanding tears the Rotator Cuff muscles may undergo atrophy, which can be seen as ‘wasting’ of the muscles over the shoulder balde (scapula). People may have a ‘painful arc’ on elevating their shoulder and positive ‘impingement signs’. People with Rotator Cuff Disease often have associated problems with Acromioclavicular Joint (ACjt) arthritis and Long Head of Biceps Tendonitis and may have symptoms and signs of these as well.
find out more about examination of the shoulder for rotator cuff disease…
-
Investigations –
-
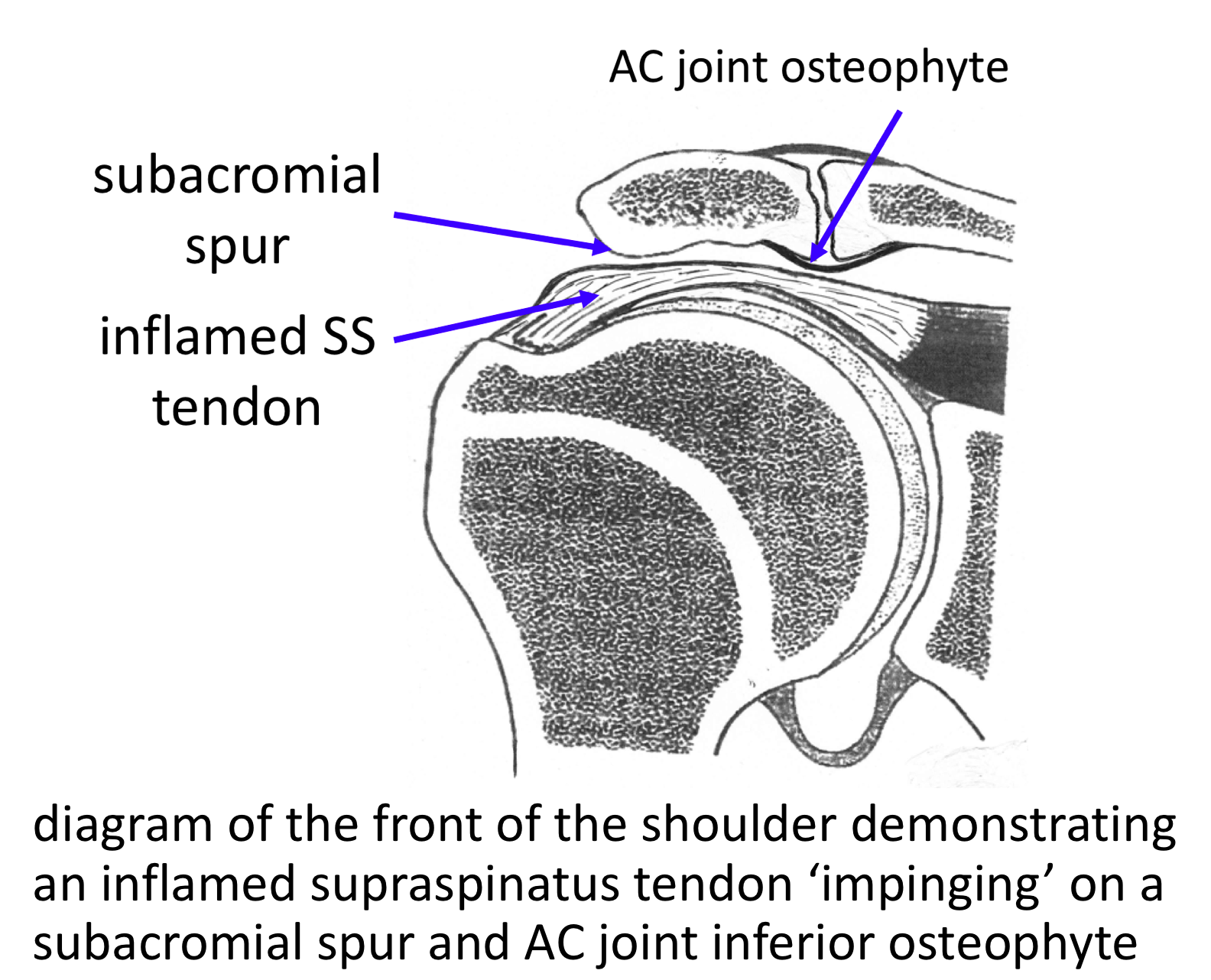
X-Ray –An x-ray does not usually demonstrate the soft-tissues of the Rotator Cuff. However, the shape of the acromion, ACjt osteoarthritis and calcific deposits can sometimes be noted.
-
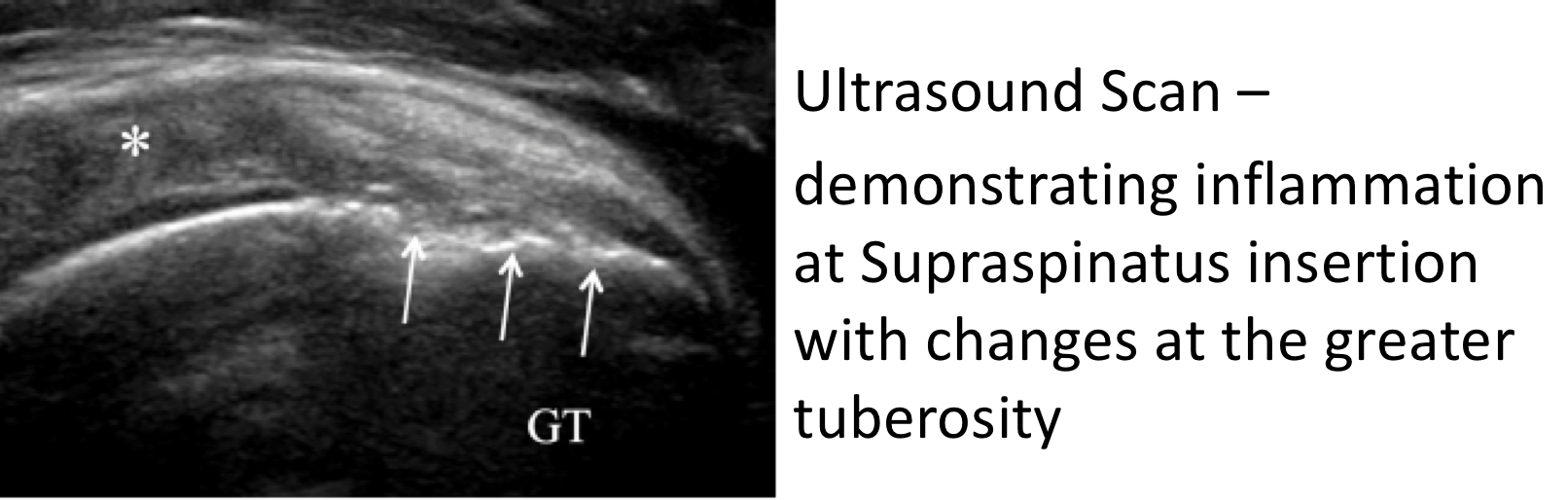
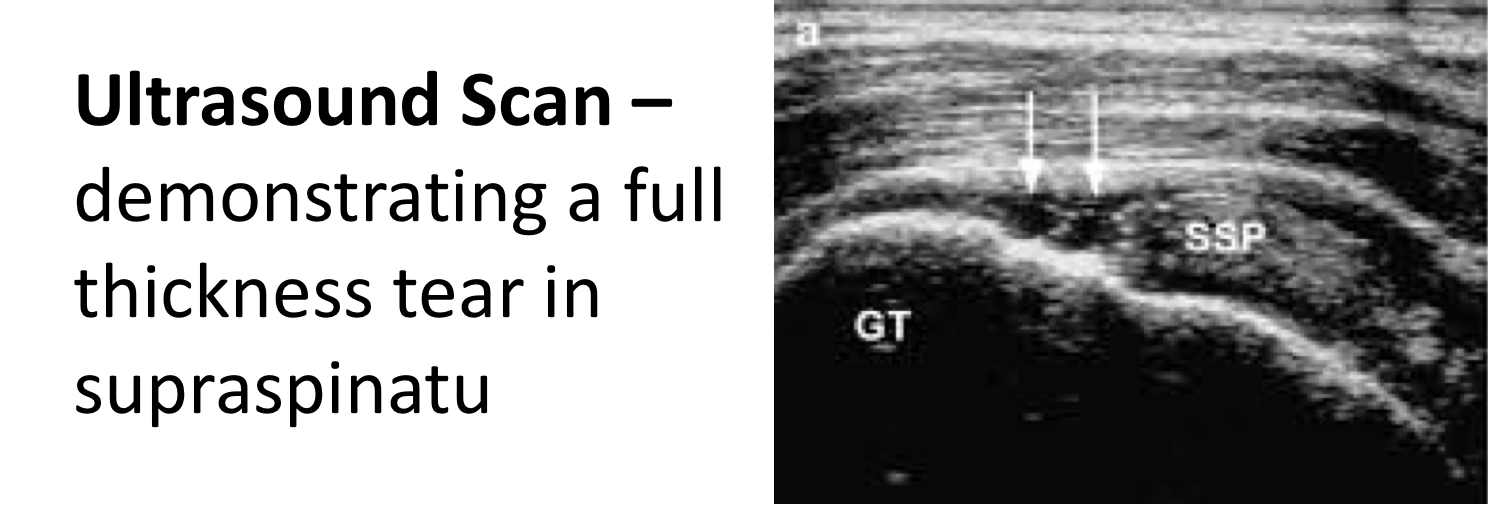
Ultrasound Scan (USS) – An USS will nicely demonstrate the Rotator Cuff tendons and the Long Head of Biceps. It is able to show whether there is a tendonitis, partial or full thickness tear of the tendons.
-
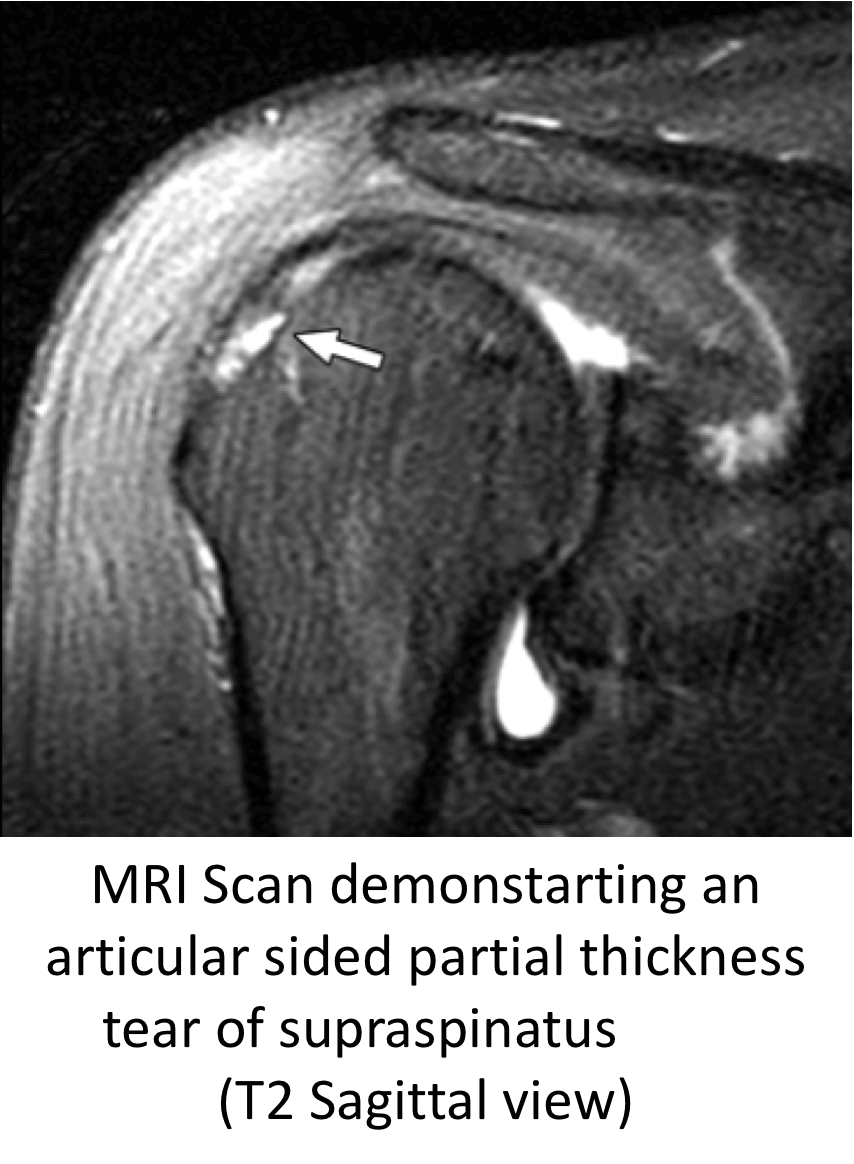
MRI Scan-An MRI scan is the best investigation to visualize the rotator cuff. It can show all of the tendons and whether there is a tendonitis, partial or full thickness tear. It will also demonstrate the acromion and ACjt and their relationship with the tendons. If there has been a longstanding tear the MRI can show evidence of how far the torn tendon has retracted and if there is any evidence of muscle belly atrophy. An MRI scan will also show up any other problems around the shoulder.
-
Management of Rotator Cuff Tears
-
There is a vast variation between the specific symptoms, types and chronicity of a tear and the needs and expectations of patients who present with a symptomatic Rotator Cuff Tear
-
There are also many different ways of treating and repairing Rotator Cuff Tears
-
My approach to treating a patient with a symptomatic Rotator Cuff Tear is to assess the specific issues and nature of their problem and to then base my recommendation of how to treat their Rotator Cuff Tear, based on this
Surgery for Rotator Cuff Tears
-
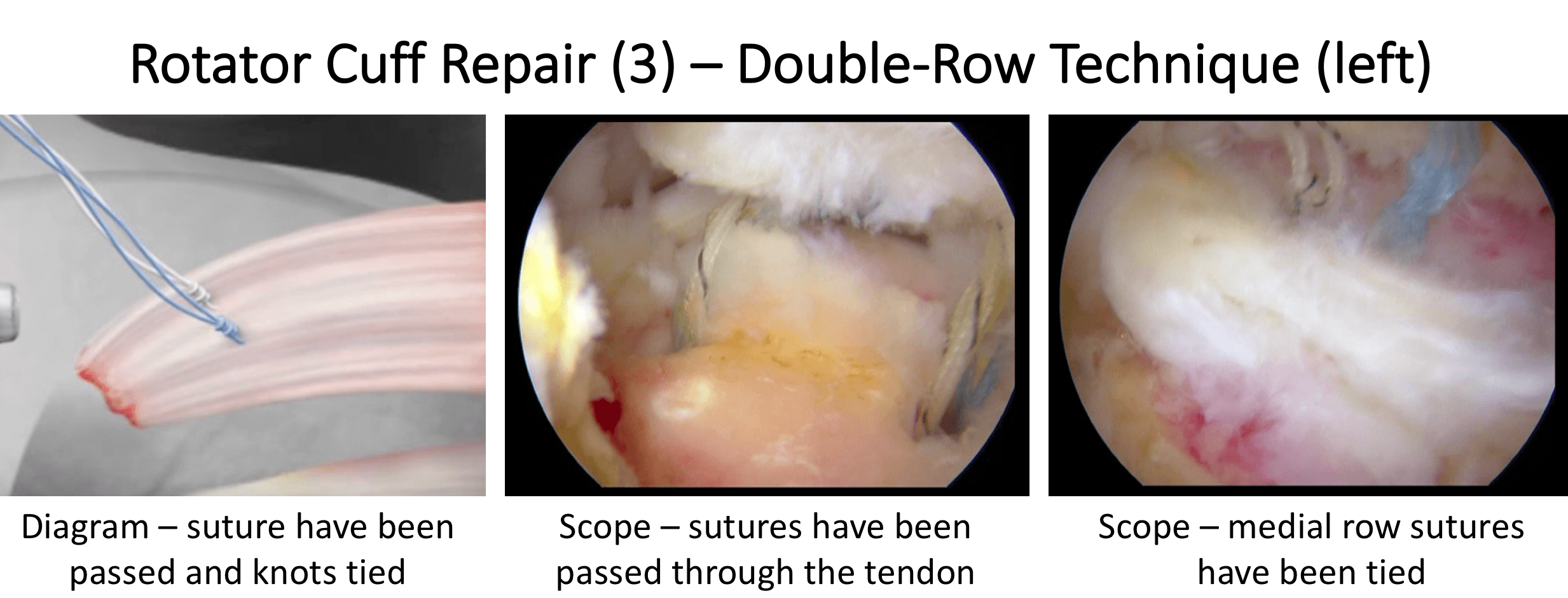
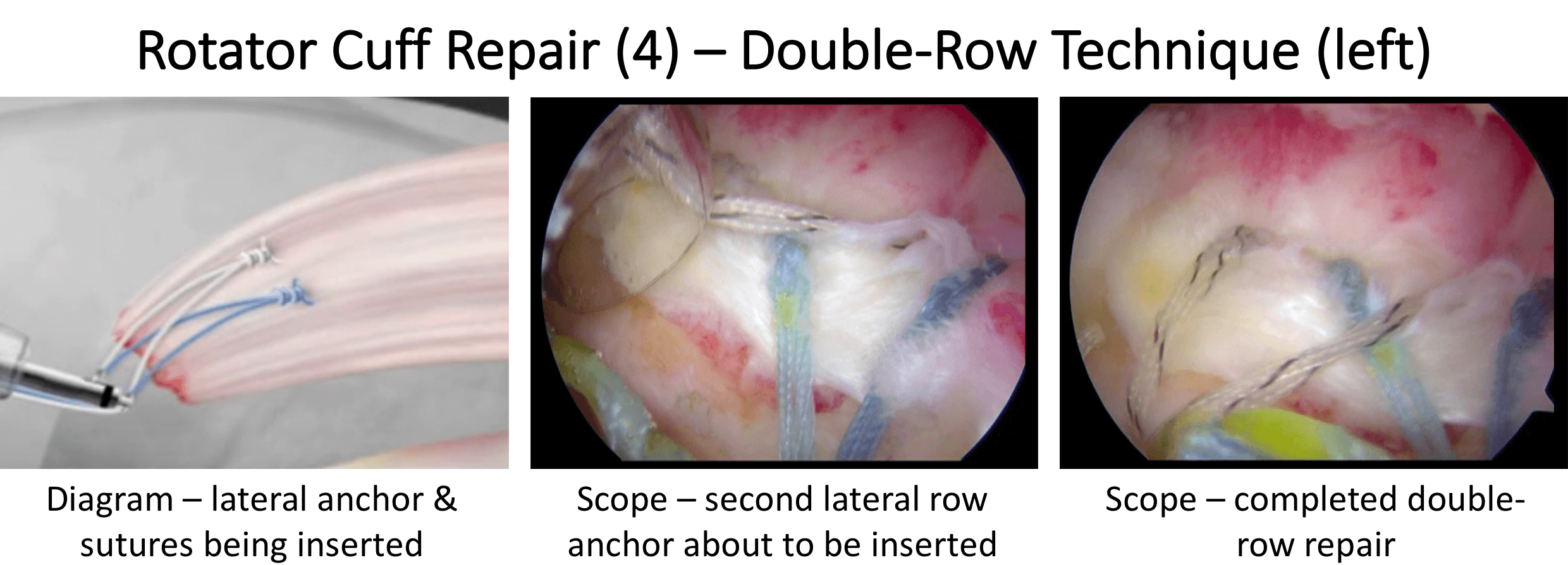
I undertake all of my Rotator Cuff Repairs using Arthroscopic Surgery (keyhole surgery)
-
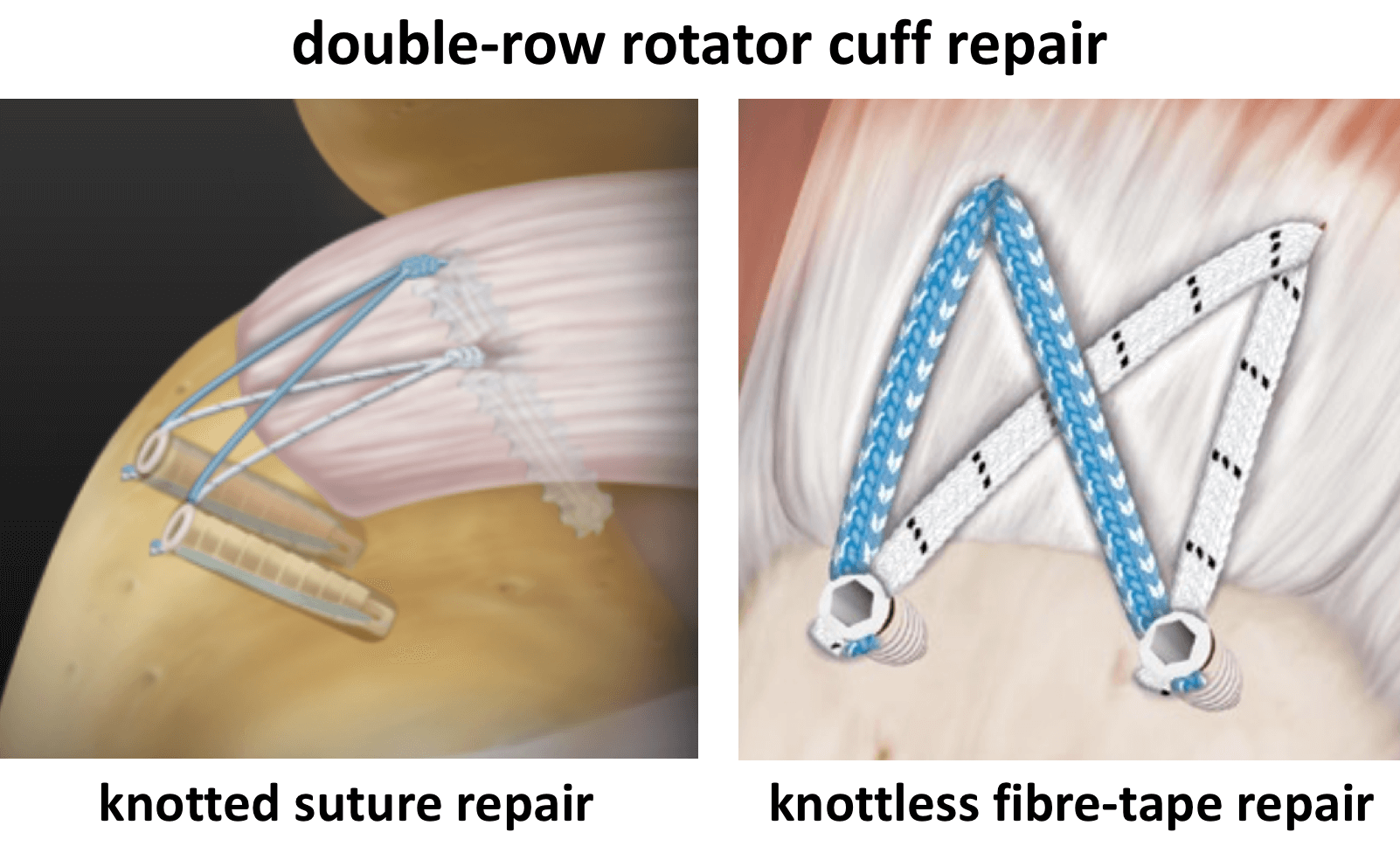
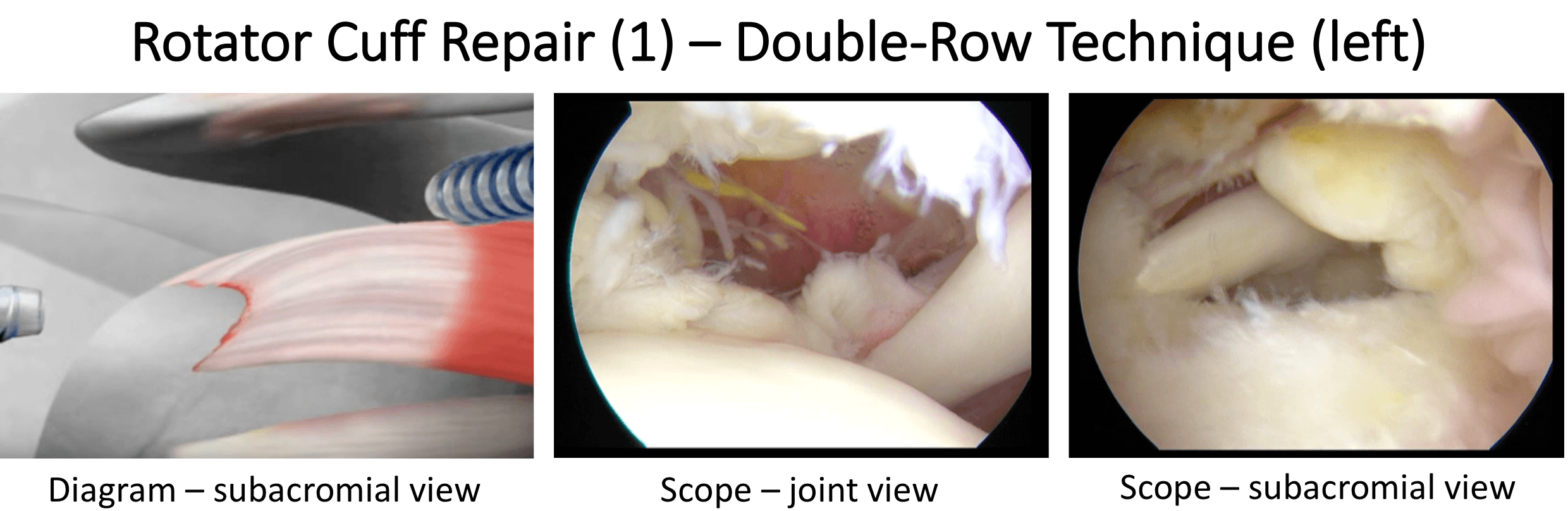
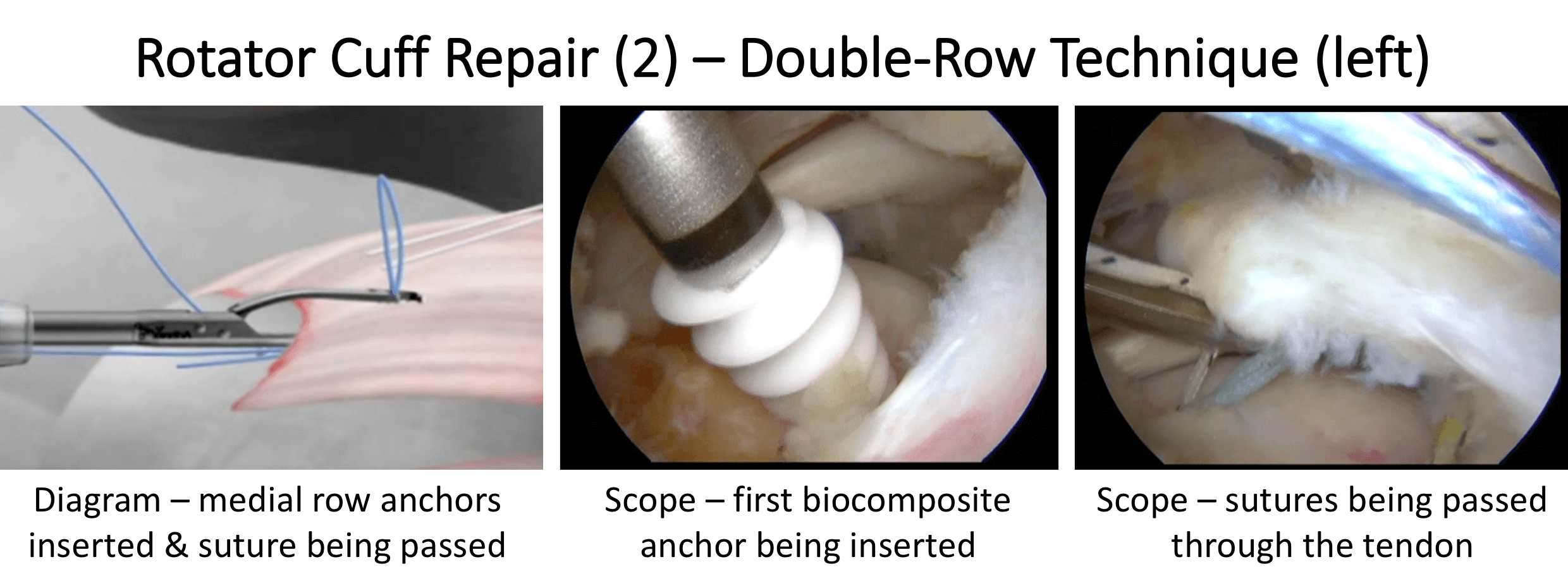
The basic aim of any Rotator Cuff Repair is to mobilise and freshen up the ends of the torn tendon, to freshen up the boney insertion on the humerus and then to position and re-attach the tendon back down to its original insertion, achieving a tensionless repair
-
To achieve this there are multiple techniques, implants and strategies that can be used
-
The descriptions of the procedures outlined below are based on the general technique. The specific details and pros and cons of the various implants and equipment that I use are covered in the Arthroscopic Surgery Section
Healing of Rotator Cuff Tears
-
Rotator Cuff Tears usually occur in tendons that have undergone ‘wear and tear’ and, as the tear occurs, the degenerate tendon is no longer strong enough to withstand the mechanical forces placed on it
-
When a Rotator Cuff Tendon is repaired it is still degenerate and, as a result, its healing potential is not as good as a normal, healthy tendon
-
Surgical techniques and implant technology are constantly advancing and we are currently able to mobilise and successfully repair nearly all tendon tears
-
However, despite this, a number of repairs still fail to heal
-
This is likely to be due to the poor healing potential of degenerate tendons
-
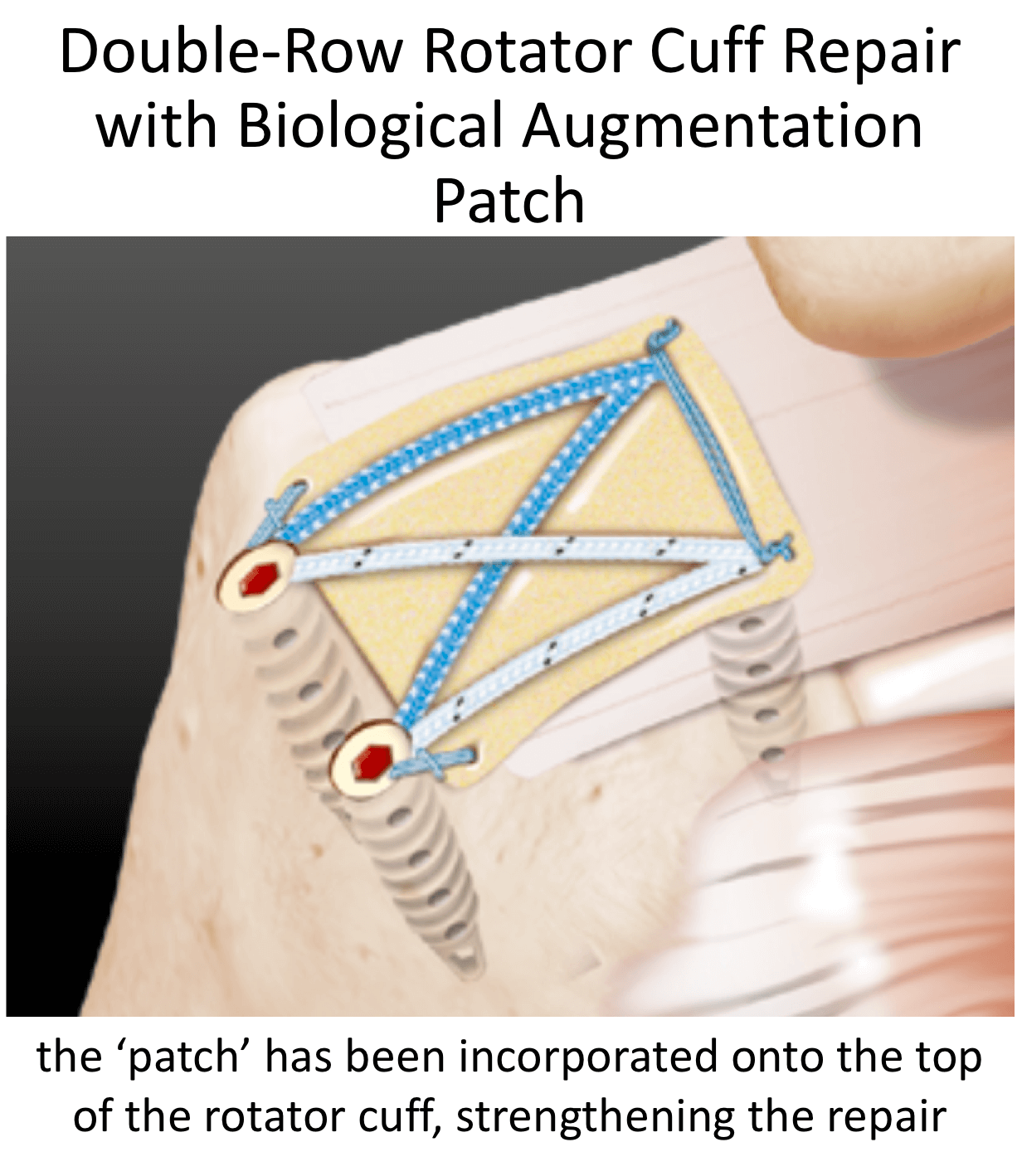
The latest advance in Rotator Cuff Repairs, ‘Ortho-Biologics’, involves trying to improve and optimize the healing potential of degenerate tendons
-
Although ‘Ortho-Biologics’ is in its infancy, it is an area where I have a great interest and I incorporate its use, where indicated, during Rotator Cuff surgery
Surgery for Rotator Cuff Tears
-
I undertake all of my Rotator Cuff Repairs using Arthroscopic Surgery (keyhole surgery)
-
The basic aim of any Rotator Cuff Repair is to mobilise and freshen up the ends of the torn tendon, to freshen up the boney insertion on the humerus and then to position and re-attach the tendon back down to its original insertion, achieving a tensionless repair
-
To achieve this there are multiple techniques, implants and strategies that can be used
-
The descriptions of the procedures outlined below are based on the general technique. The specific details and pros and cons of the various implants and equipment that I use are covered in the Arthroscopic Surgery Section

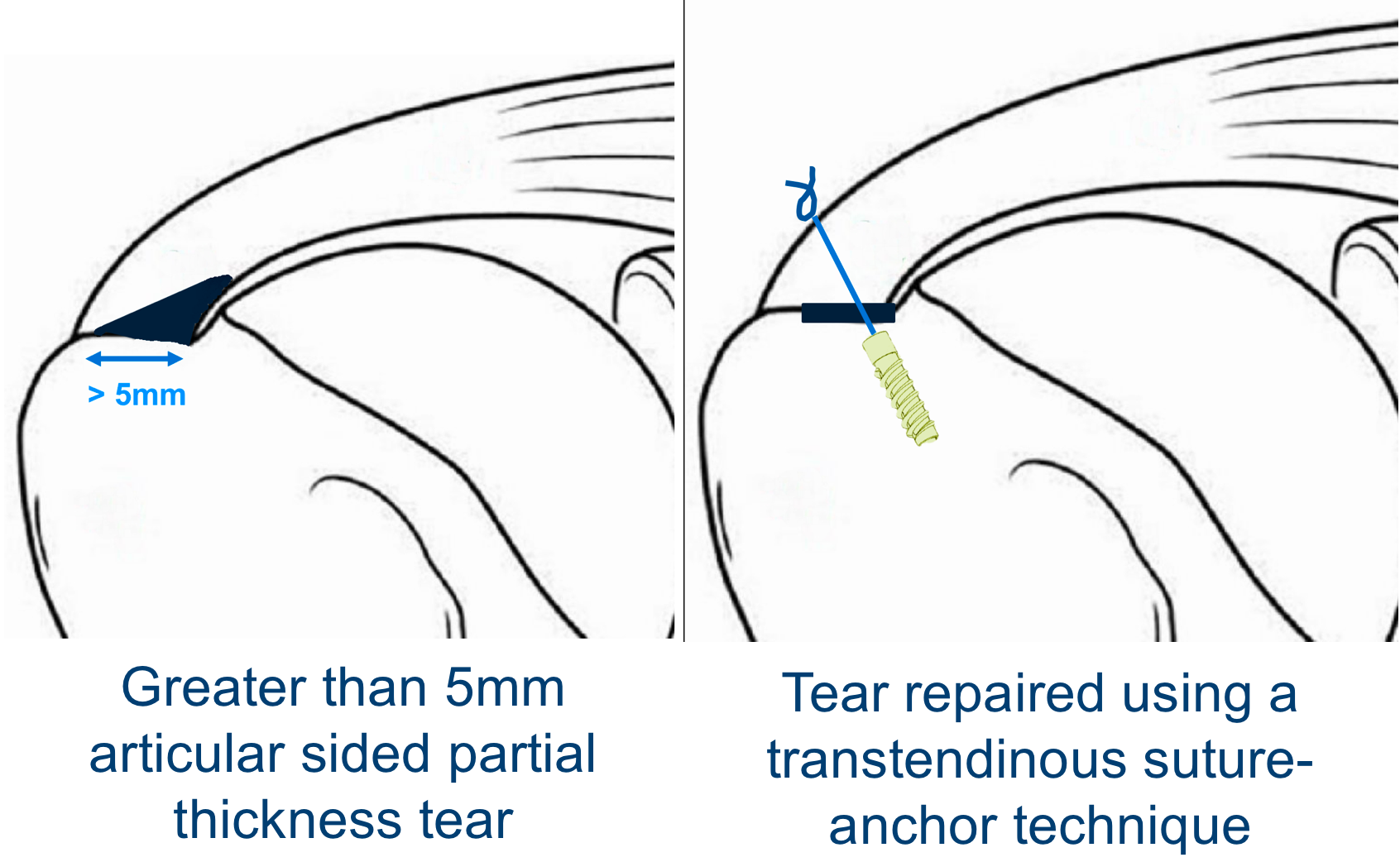
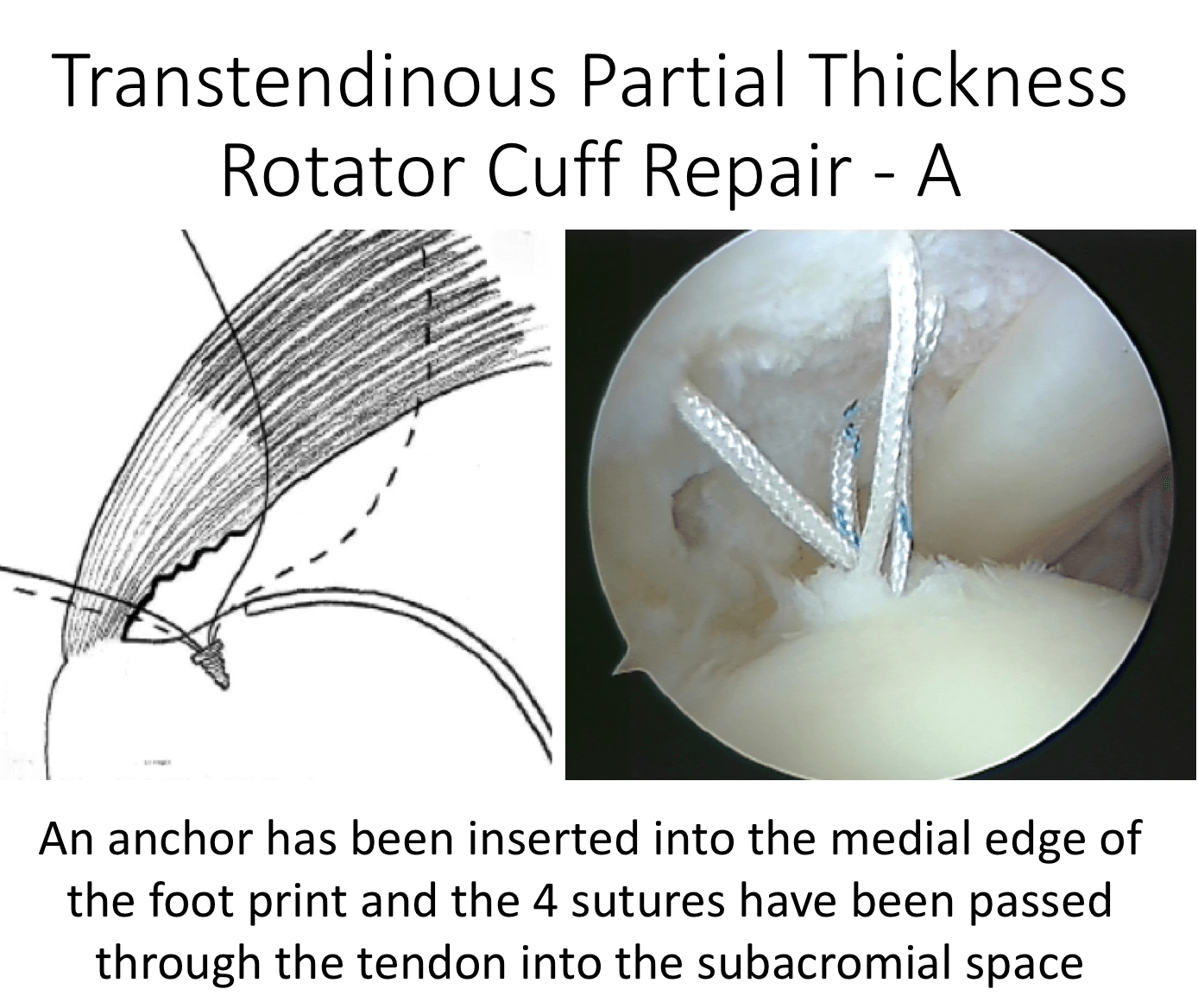
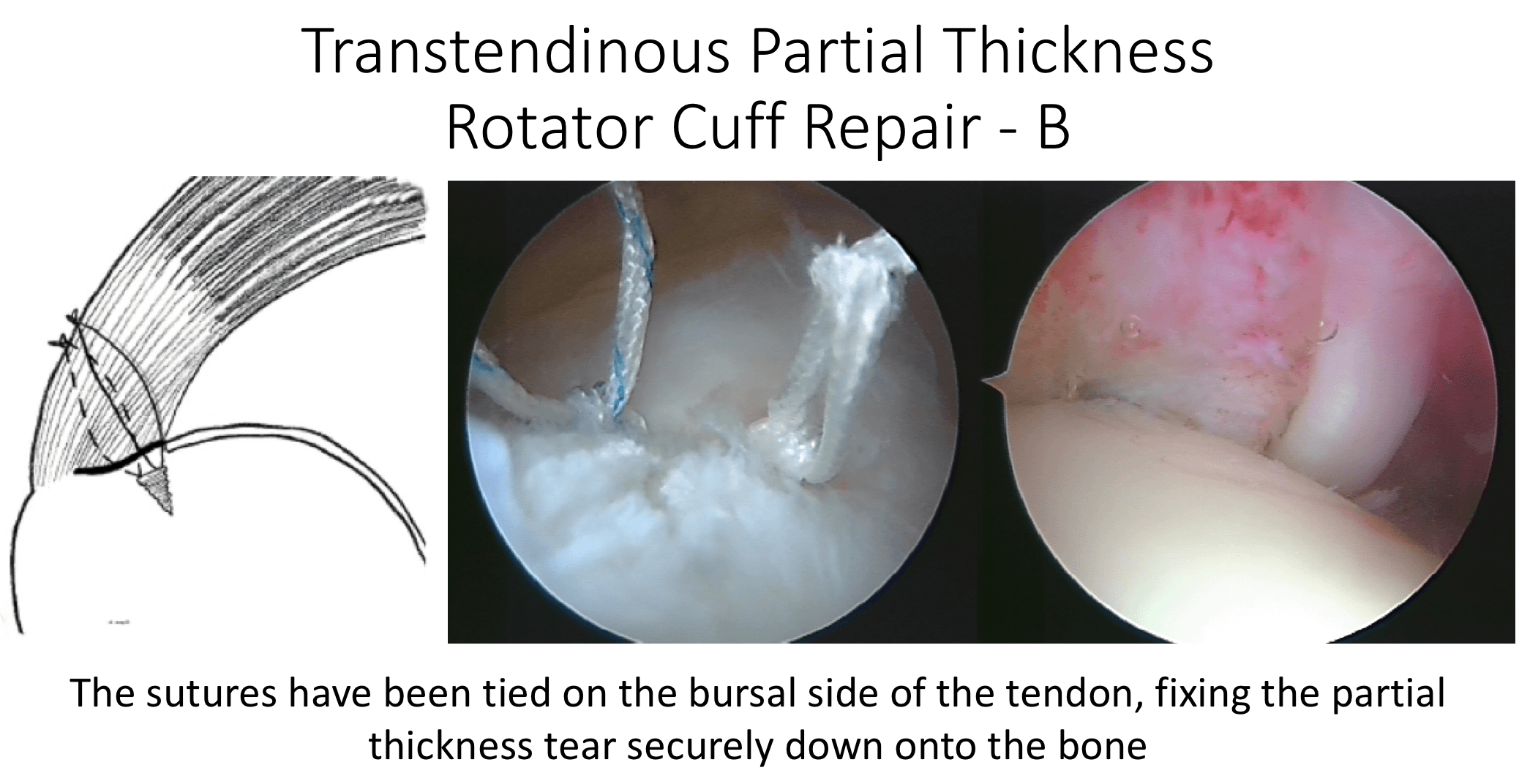
Depending on the exact position and size of the Partial Thickness Tear, the tendon can either be repaired using a transtendinous technique. If the tear as almost completely through the tendon it can be converted into a Full Thickness tear and then be repaired in that way. The specific implants that are used can also vary depending on certain technicalities and using implants that are the most appropriate. My routine Arthroscopic Trans-Tendinous Partial Thickness Rotator Cuff Repair Procedure is described below,

Arthroscopic Rotator Cuff Repair


watch a video of a Rotator Cuff Repair …
Find out more about arthroscopic surgery….
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
- A single prophylactic dose of broad-spectrum anti-biotics is administered
- A posterior, 1 – 2 anterior and 1 – 2 lateral portals are used to access the Gleno-Humeral Joint (Shoulder Joint) and Subacromial spaces

Arthroscopic Debridement (for Irreparable Rotator Cuff Tears)
An Arthroscopic Debridement is aimed at tidying up and removing all of the debris and damaged tissue from around the shoulder. It is primarily aimed at pain relief but often, as a result of reducing the level of pain, the patient’s shoulder function can be improved. In some cases, the Long Head of Biceps tendon, where it is still present, can be an additional source of pain and a Tenotomy (release of the tendon) may be of benefit. In other instances a component of someone’s pain may be due to irritation of the Suprascapular Nerve, addressing this with a Nerve Release or Ablation may also be of benefit. Both of these procedures can be done at the same time as an Arthroscopic Debridement.
An Arthroscopic Debridement is a relatively small procedure which can often be done as a Day-Case. The shoulder does NOT need to be immobilised after the surgery and patients can often notice an improvement fairly quickly.
However, like most operations for Irreparable Rotator Cuff Tears, results can be variable and it is not usually possible to predict how much any one person is likely to benefit from surgery until it has be done. My routine Arthroscopic Trans-Tendinous Partial Thickness Rotator Cuff Repair Procedure is described below,
find out more about the Suprascapular nerve….
Find out more about Arthroscopic Surgery….
Watch a video of an arthroscopic debridement of the shoulder….
Arthroscopic Debridement (+/- Biceps Tenotomy & Suprascapular Nerve Ablation)
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
- A posterior, anterior and 1 – 2 lateral portals are used to access the Gleno-Humeral Joint (Shoulder Joint) and Subacromial spaces
- The Glenohumeral Joint is initially viewed to assess the size and extent of the tear and to look for any other associated problems, particularly with regards to Osteoarthritic changes to the joint and problems with the Long Head of Biceps
- Using a Shaver and Radiofrequency wand the joint is then cleaned out removing any loose fragments and excising any ragged tissue
- If the Long Head of Biceps is considered to be damaged a Tenotomy is performed
- The Subacromial Space is then entered and, using the Shaver and Wand, the stump of the torn Rotator Cuff Tendons are tidied up and any other ragged tissues excised
- If the Suprascapular is considered to be a source of pain it is exposed using an accessory Nervaiser type portal. The nerve is then either released or ablated
- At the end of the procedure the joint and subacromial space are assessed, washed out and the wounds closed with sub-cuticular sutures
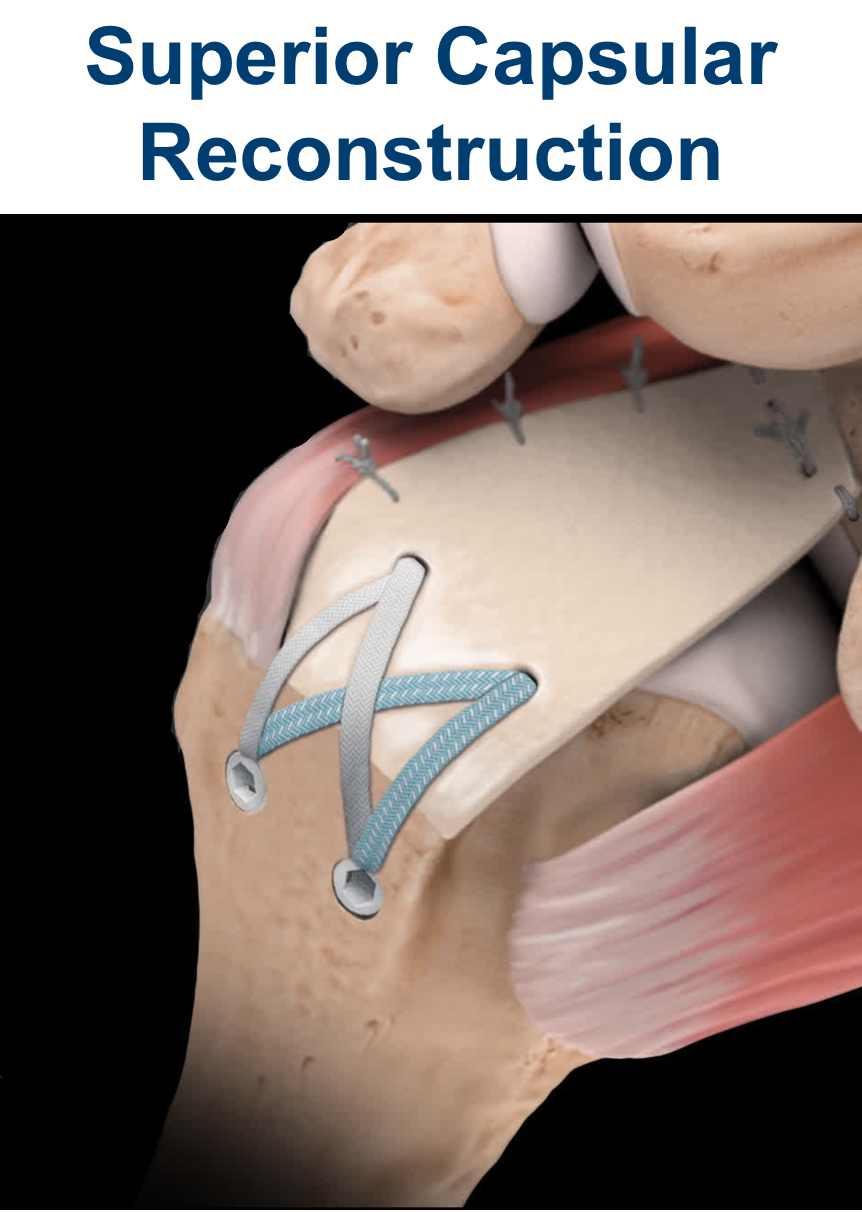
Previously there were really no reliably successful surgical procedures available to improve ‘function’ for patients with a symptomatic Irreparable Rotator Cuff Tear. Although it is relatively early days, a Superior Capsule Reconstruction appears to be able to achieve this, certainly initially, when performed correctly on appropriate patients. I, personally, have been very pleased and impressed with the initial outcomes using this procedure on a limited number of patients. However, it is a new procedure and, as of yet, we do not know what will happen with patients’ shoulders over a longer time.
My routine Superior Capsule Reconstruction Procedure is described below…
