Calcific Tendonitis
Calcific Tendonitis refers to calcium deposits forming in the rotator cuff tendons (most commonly the – Supraspinatus Tendon). Although, most of the time, calcific deposits are small and do not cause any pain, they can occasionally cause very significant problems. This can be due to a deposit causing pressure and mechanical symptoms and to chemical ‘irritation’.
There are 2 types of Calcific Tendonitis
Degenerative Calcific Tendonitis
- Degenerative Calcific Tendonitis can occur as part of normal degenerative wear and tear in rotator cuff tendons when some of the fibres begin to fray and wear. During the healing process calcium deposits are sometimes formed within the damaged tendons.
- This is often an ‘evolving process’ so that, over time, these calcium deposits form and are then slowly resorbed.
- this process is very common between the ages of 30 to 60 years, and is often painless, so that most of the time it is asymptomatic and people do not know that it is going on.
- calcific deposits can often be seen on plain x-rays, and it is estimated that 5% of the population between 30 to 60 years of age will have a calcium deposit on a shoulder x-ray, despite being asymptomatic.
- however, in certain people, the calcium deposit can become very large and lead to significant pain due to pressure within the tendon, impingement and chemical ‘irritation’.

Reactive Calcific Tendonitis
- Reactive Calcific Tendonitis is a different process and is not related to degeneration. The cause is not known, but it appears that, due metabolic changes within the tendon, calcium deposits are formed.
- As the deposits begin to form there can be a rapid increase in ‘pressure’ within the tendon, sometimes leading to an acute onset of severe pain
- Again, this is an ‘evolving’ process and over time the calcium deposits and are slowly resorbed.
- This process is relatively uncommon but can occur in people from the age of 20 to 60 years.
What are the Symptoms of Calcific Tendonitis
Chronic / Degenerative Calcific Tendonitis
- The symptoms of Chronic Calcific Tendonitis are identical to those of supraspinatus tendonitis or impingement
- In fact the cause of the pain is identical as essentially the enlarged and inflamed tendon impinges on the undersurface of the acromion
- As degenerative calcific deposits form slowly the onset of symptoms can often be quite insidious. As a result, many people find that Calcific Tendonitis gradually develops over time..
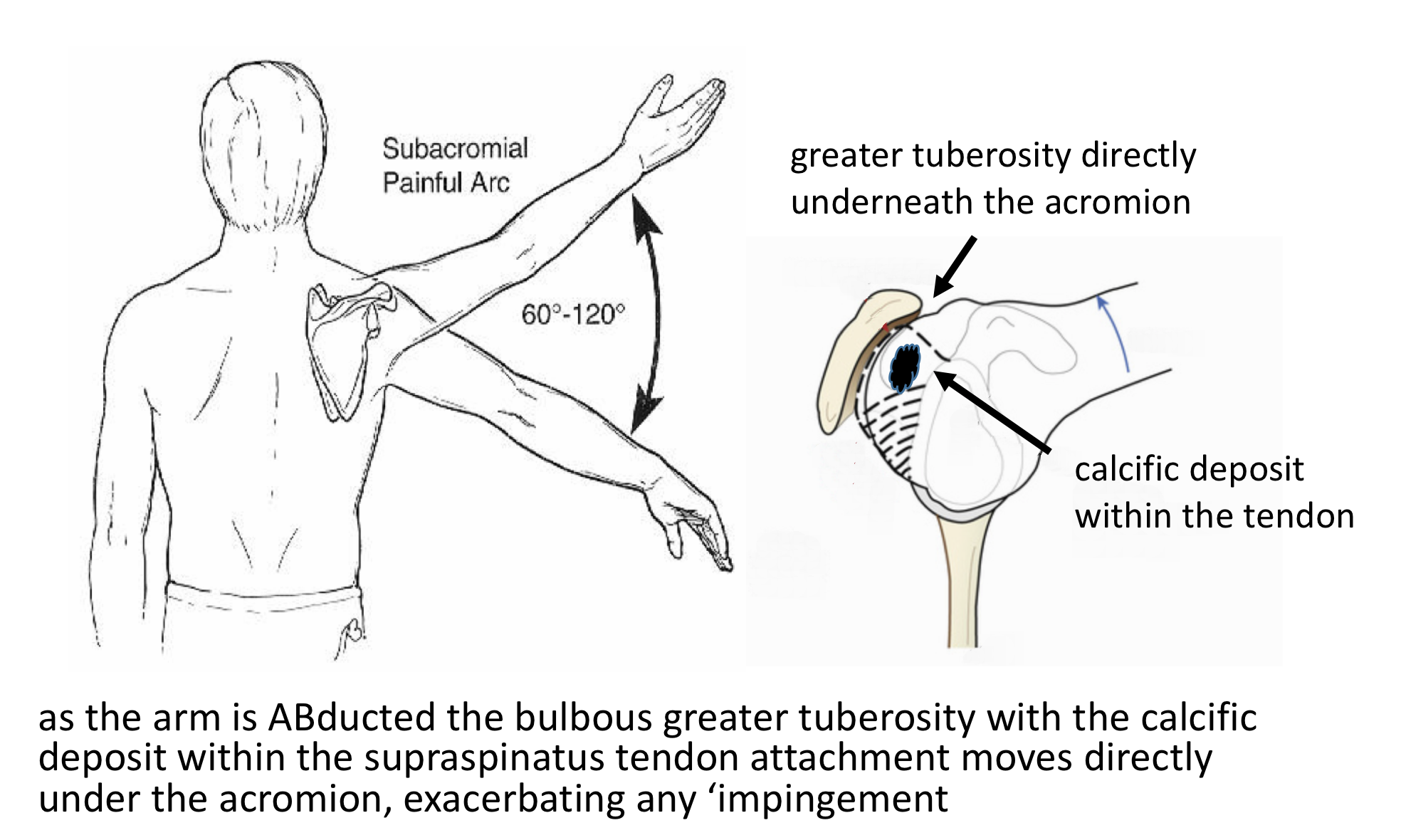
- There is a bulge on the side of the Humeral Head (Greater Tuberosity) where the Supraspinatus and Infraspinatus Tendons insert into the bone. As the shoulder moves, this bulge lies directly under the acromion between 60 and 120 degrees of elevation. This is the point where the space between the top of the Humeral Head and the Acromion is the narrowest. This is known as the ‘Painful Arc’ of movement. The early symptoms of Calcific Tendonitis tend to be a background pain over the shoulder with particular discomfort when elevating the shoulder within the ‘Painful Arc’. The shoulder is often uncomfortable to lie on at night.
- As symptoms deteriorate the shoulder becomes increasingly painful more of the time. Pain tends to occur on more directions of movement and the shoulder can appear to become weaker. Night discomfort often becomes more of a feature.
Acute / Reactive Tendonitis
- In Acute Calcific Tendonitis the calcific deposits usually form rapidly
- Symptoms can occur suddenly ‘out of the blue’ or maybe precipitated by a minor injury
- Sometimes, within a matter of hours, patients develop an ‘excruciating’ pain that is there constantly
- The pain can be so severe that even the strongest pain-killers do not seem to have an effect
How do you Diagnose Calcific Tendonitis?
- History – Most people notice a gradual onset of pain and discomfort over the top and side of their shoulder. Sometimes people can identify a specific injury or incident that triggered their problem. They may notice particular pain on elevating their arm and in bed at night. As the condition deteriorates they may get pain more of the time and on more directions of movement. They also might notice some weakness.

- Examination – Patients often experience some discomfort on palpation over the front edge of their Acromion directly over the insertion of the supraspinatus tendon, where the calcific deposit lies. People may have a ‘painful arc’ on elevating their shoulder and positive ‘impingement signs’. People with Supraspinatus tendonitis often have associated problems with Acromioclavicular Joint (ACjt) arthritis and Long Head of Biceps Tendonitis and may have symptoms and signs of these as well.
find out more about examination of the shoulder for rotator cuff disease…(Research & Education – Video – Examination of the Shoulder 3)

- Investigations – Chronic Calcific Tendonitis
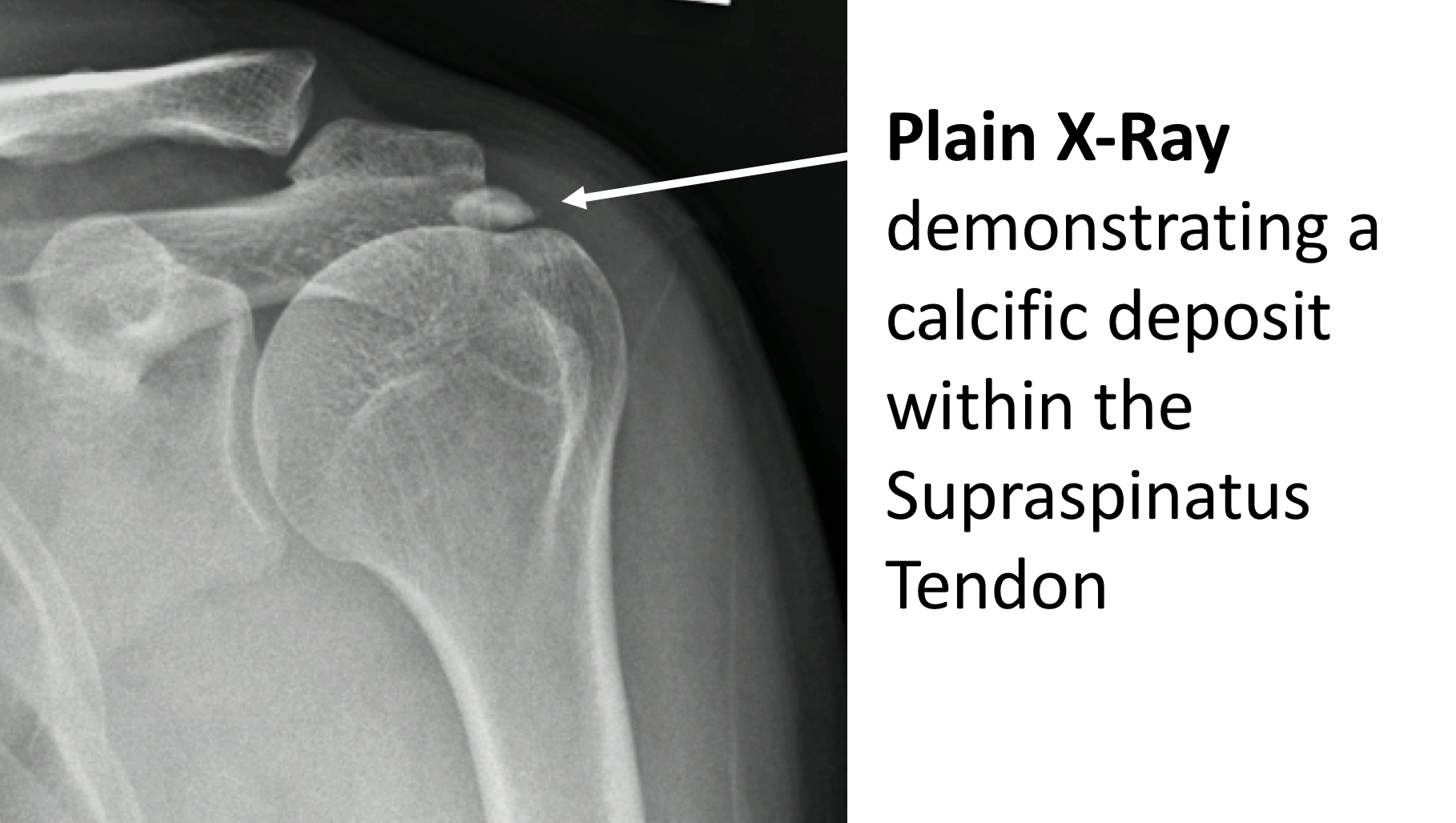
- X-Ray –For Chronic Calcific Tendonitis an x-ray will usually demonstrate a calcific deposit sitting in the space underneath the acromion. This is where the supraspinatus tendon is situated.
find out more about x-rays…. (Patient Information – Imaging – X-Rays)
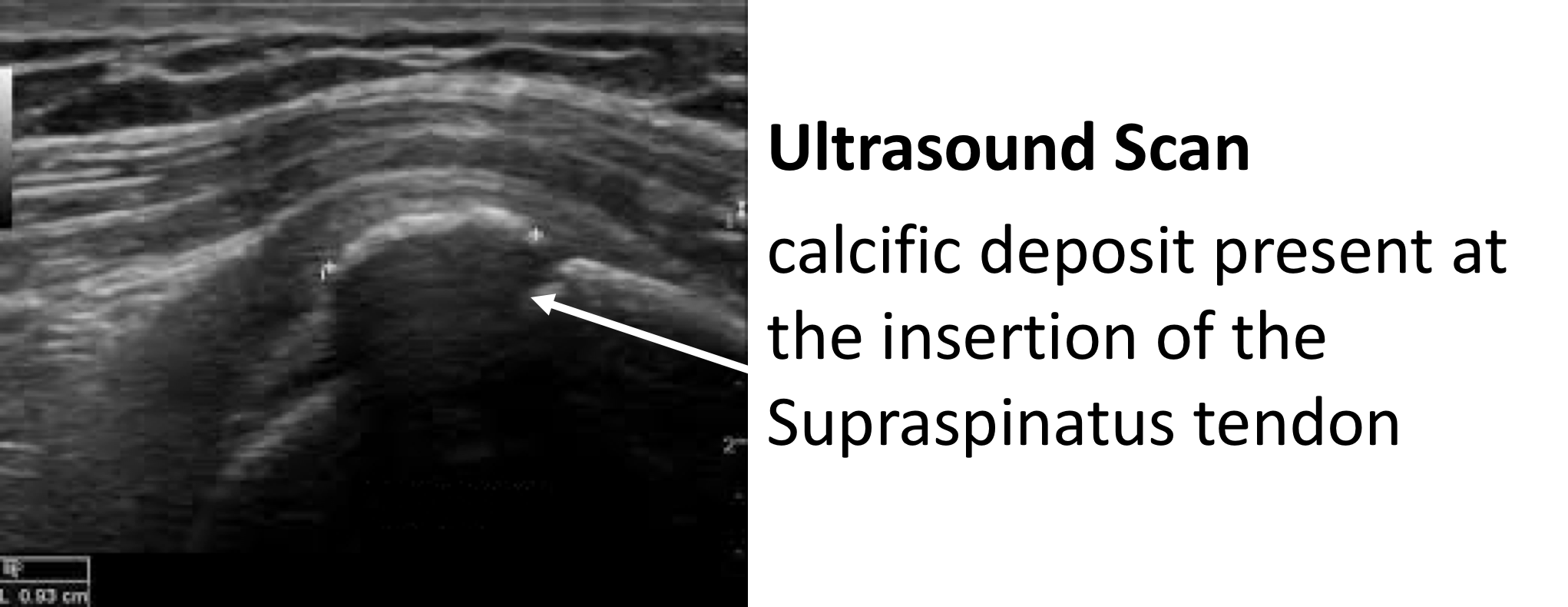
- Ultrasound Scan (USS) – An USS will nicely demonstrate the Rotator Cuff tendons and the Long Head of Biceps. It is able to show a Calcific Deposit and whether there is an associated tendonitis, partial or full thickness tear of the tendons.
find out more about USS….(Patient Information – Imaging – USS)
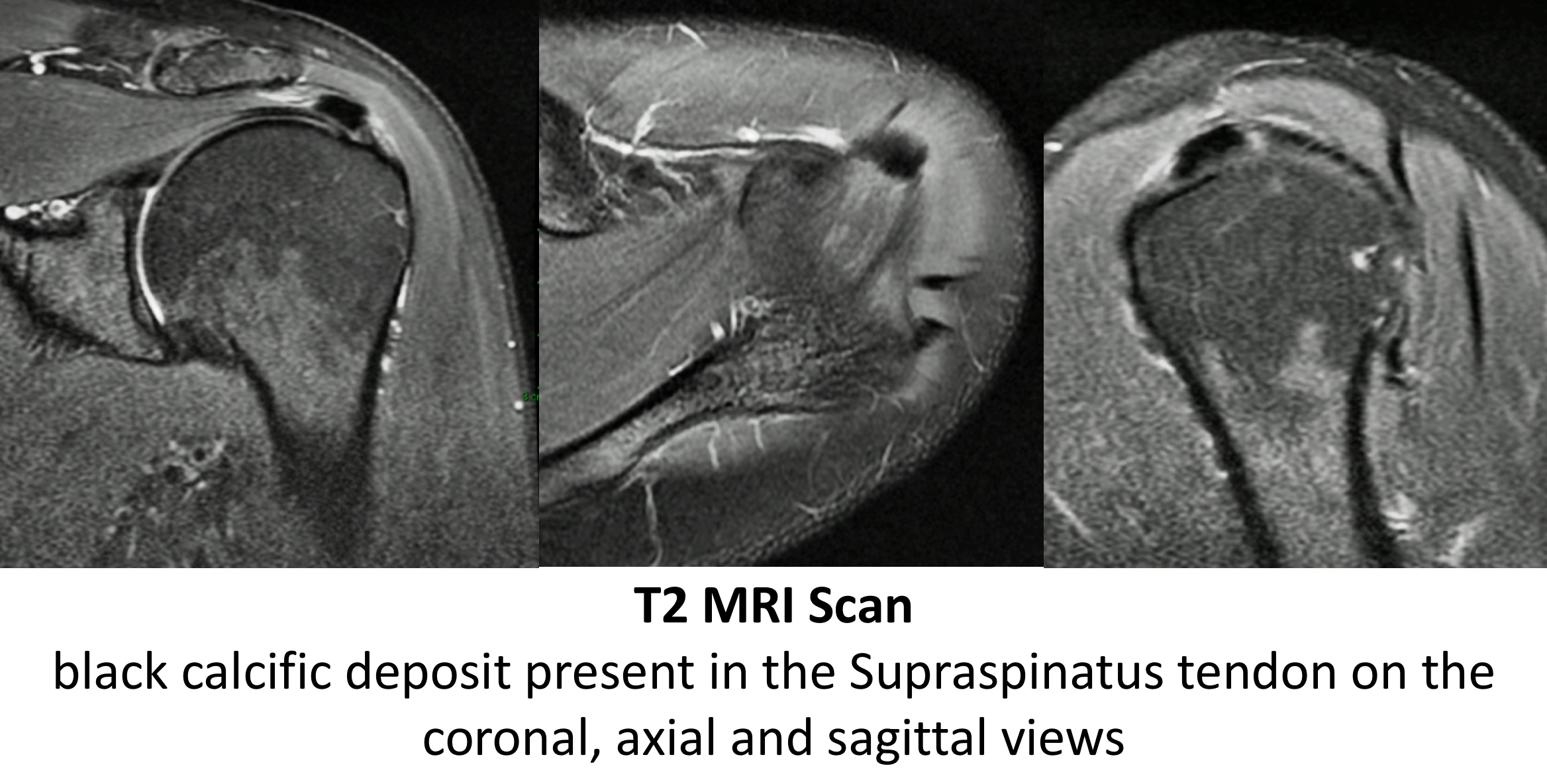
- MRI Scan- An MRI scan is the best investigation to visualize the rotator cuff. It can show all of the tendons and whether there is a calcific deposit, tendonitis and a partial or full thickness tear.
Find out more about MRI scans….(Patient Information – Imaging – MRI)
- Investigations – Acute Calcific Tendonitis
- The symptoms of an Acute Calcific Tendonitis can develop so rapidly that insufficient calcium deposits may have been formed to be visualized on an X-Ray or an Ultrasound Scan in the early stages
- MRI Scan- An MRI scan is the best investigation to visualize the early changes associated with an Acute Calcific Tendonitis
Management of Chronic Calcific Tendonitis
The vast majority of patients with a Chronic Calcific Tendonitis can be successfully treated non-operatively with a combination of NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) and Physiotherapy. The treatment is identical to that for Supraspinatus Tendonitis
- Physiotherapy – Physiotherapy and specific Rotator Cuff Strengthening exercises are the main-stay of the initial treatment for Chronic Calcific Tendonitis. By specifically strengthening the Supraspinatus muscle, where the deposit is usually located, it can work and contract more efficiently pulling the humeral head downwards and allowing the tendon to move more freely. If pain is a particular feature a short course of NSAIDs prescribed by a Physician can help.
find out more about Rotator Cuff Strengthening Exercises….(Patient Information – Physiotherapy – Physiotherapy-Rotator Cuff – Non-Operative)

- Analgesia/Pain Relief
- NSAID (Non-Steroidal Anti-Inflammatories) –
- NSAIDs work be reducing the painful inflammatory response
- NSAIDs can damage the stomach lining and affect the kidneys. It is important that a patient’s Family Doctor prescribes this medication if it is going to be used for a longer term
- Codeine based Analgesics –
- Codeine based analgesics are pain killers and affect a patient’s perception of pain. As a result, they can have some effect on consciousness depending on their strength
- Codeine based analgesics can lead to constipation if taken for a longer time. Having a high-fibre diet or even taking laxatives might need to be considered
- Nociceptive Analgesics –
- Nociceptive pain killers work on nerve generated pain
- Amitriptyline in lower doses works as a nociceptive pain killer. It has a useful side-effect in that it can make patients drowsy
- in cases of severe pain Amitriptyline can be prescribed at night
- NSAID (Non-Steroidal Anti-Inflammatories) –

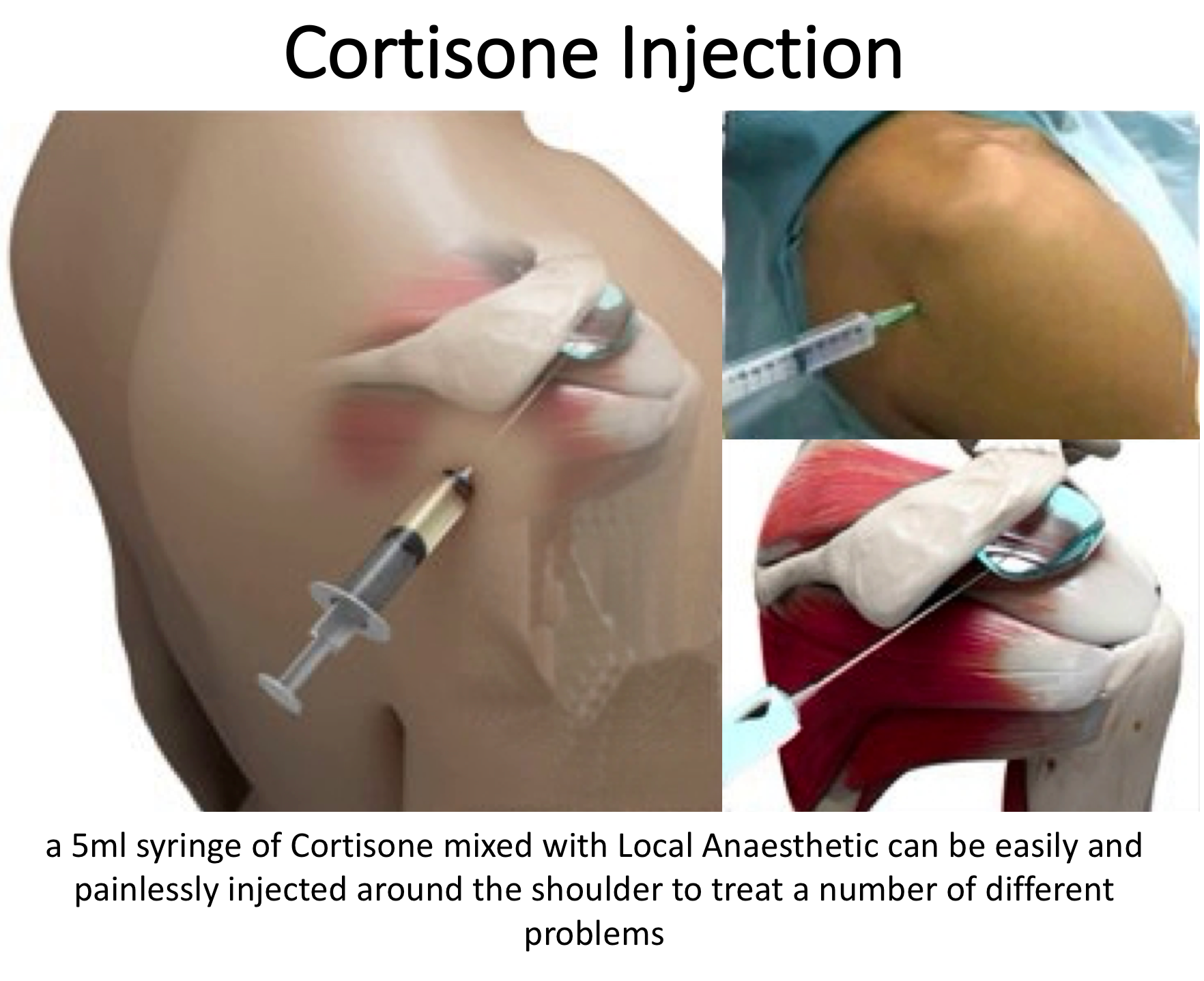
- Subacromial Cortisone Injection –
- If someone’s Chronic Calcific Tendonitis has failed to settle, after an adequate course of Physiotherapy, a Subacromial Cortisone injection can help to settle the symptoms down. Cortisone is a corticosteroid that is naturally produced by the body’s Adrenal Gland. Injectable Cortisone is synthetically produced and has a very powerful ant-inflammatory action. When injected into the Subacromial space it has the potential of settling severe inflammation, allowing the patient to undertake their rehabilitation exercises.
- A Subacromial Cortisone can be easily administered in the Out-Patient Clinic. It is a quick and relatively painless procedure. Afterwards patients can continue with their normal day-to-day activities. Occasionally patients can feel a bit of soreness around their shoulder later that day, but this usually passes fairly quickly
- It often takes several days before someone notices the benefits following a Cortisone injection and sometimes several weeks. The Cortisone works in the background and there is no specific requirement to particularly rest the shoulder or to do extra exercises. The full benefits of a Cortisone injection are usually felt within a month. In some cases, the Cortisone may not give any benefit, this may be an indication of the severity of the Supraspinatus Tendonitis.
- A Cortisone injection only lasts in the body for a few days. Any benefit that someone gets from the Cortisone will be from its acute anti-inflammatory effect allowing the Supraspinatus Tendonitis to settle. If the symptoms do return after a while, it is not because the Cortisone has worn off, but because the inflammation has returned.
- Infections can occur after any type of injection but are extremely rare (1 in 15,000). If someone feels that they are developing an infection within 48 hours of a Cortisone injection they should seek advice from their Family Practitioner.
- Surgery for Chronic Calcific Tendonitis – In some instances a Supraspinatus Tendonitis fails to respond, or continues to recur, despite adequate Physiotherapy and Cortisone treatment. In this situation the only treatment that is likely to settle the symptoms is Surgery.

Arthroscopic Subacromial Decompression, Excision of Calcific Deposit +/- Rotator Cuff Repair
The best operation for someone with a Chronic Calcific Tendonitis, that is refractory to treatment, is an Arthroscopic Subacromial Decompression and excision of the calcific deposit. This is an operation where an Arthroscopic camera is positioned inside the Subacromial Space and, by using specialized instruments, the undersurface of the front of the acromion is burred away. This creates more space for the Supraspinatus Tendon to run underneath the Acromion.

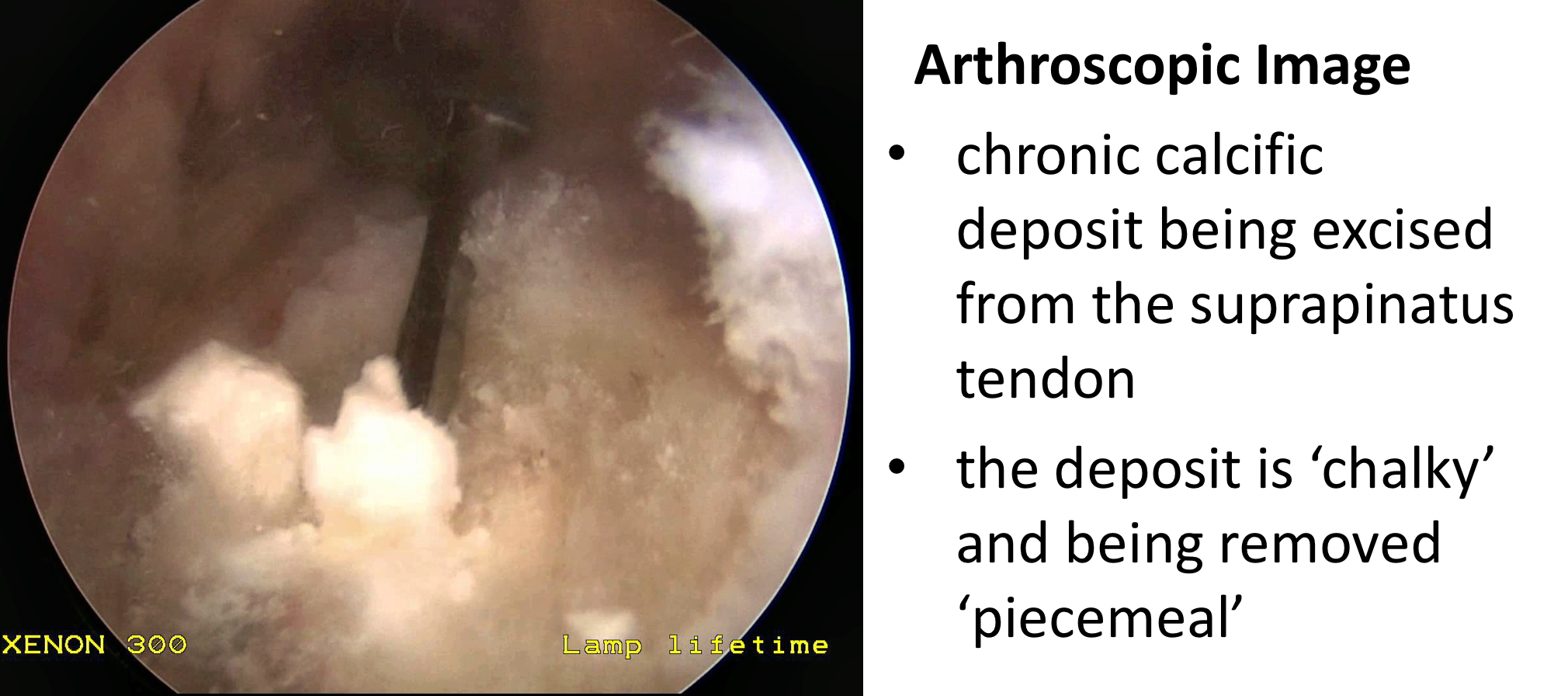
Following this the Calcific Deposit can be identified and removed. The deposit is usually of a chalky consistency within the tendon. So rather than being able to extract it as a single lump, it is usually the case of removing as many bits as possible. To do this, depending on the size of the deposit, may involve opening up the tendon which can result in a defect or hole being left behind. If this is the case a Rotator Cuff Repair is then undertaken.
An Arthroscopic Subacromial Decompression and Excision of Calcific deposit can usually be done as a Day Case procedure and the patient’s shoulder does not need to be immobilized for anytime afterwards, unless an additional rotator cuff repair has been undertaken. The surgery aims to remove the part of the Acromion and the calcific deposit that has been causing pain. It does not instantaneously deal with the underlying inflammation. However, by enabling the Supraspinatus Tendon to run freely and removing the deposit the symptoms can then begin to settle down. As a result it usually takes between 3 – 6 months to gain the full benefits of the procedure. It has a high success rate with around 95% of patients being happy with the result 6 months after their operation. My routine Arthroscopic Subacromial Decompression and Excision of Calcific Deposit Procedure is described below,
Watch a video of an Arthroscopic Subacromial Decompression…(Research & Education – Video – Subacromial Decompression)
Find out more about arthroscopic shoulder surgery….
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
- A posterior and a single lateral portal are used for to view the Gleno-Humeral Joint (Shoulder Joint) and Subacromial spaces
- The Glenohumeral Joint is initially assessed to look for any other problems that might be associated with a Supraspinatus Tendonitis and, in particular, the Rotator Cuff and the Long Head of Biceps
- The Subacromial Space is then entered and the undersurface of the Acromion identified.
- A lateral portal is then created
- Using a combination of a powered shaver and radiofrequency probe the coracoacromial ligament is released, revealing the Subacromial Spur.
- A powered burr is then used to resect about 5mm of bone from the undersurface of the acromion
- The Decompression is then assessed to check that sufficient bone has been resected to alleviate the Impingment
- The Rotator Cuff is then examined and the Calcific Deposit identified
- Using a combination of a probe, punch and shaver the chalky Calcific Deposit is then removed
- After removal of the Calcific Deposit the Rotator Cuff Tendon is assessed and, if there is a significant defect, this will be then also be repaired
- The Subacromial Space is then washed out and the wounds closed with sub-cuticular sutures
After the Surgery
Post-Operative Care
Following an Arthroscopic Subacromial Decompression the patient is usually able to go home on the same day as their surgery. I would see the patient after the surgery to discuss how the procedure has gone and arrange for further Follow-Up. The patient will be seen by the In-Patient Physiotherapy team, who will instruct them on the initial Rehabilitation Protocol for their shoulder. Further Out-Patient physiotherapy will then be organised.
Find out more about Physiotherapy following an ASD….
I would usually review patients in the clinic 1 month and 3 months after their procedure to assess their progress and recovery.
Rehabilitation Protocol
Immediately after the surgery, when the patient has woken up from their general anaesthetic, their shoulder and arm will be numb from the interscalaene nerve block. This will usually last for 18 – 24 hours after the surgery. For this period, we advise patients to keep their arm in a sling, purely for protection. After the nerve block has worn off the arm can begin to be taken out of the sling. I encourage patients to wean themselves off of using the sling as quickly as possible, within the limits of discomfort.
My standard rehabilitation protocol is outlined below for a standard procedure WITHOUT an additional rotator cuff repair. The information and time to recovery are a general estimation and may vary from person to person.

|
Post op |
|
| Immediate |
|
| Day 1-3
Weeks |
|
| 3-6 Weeks |
|
|
Milestones |
|
|
Week 3 |
Full passive range of movement |
|
Week 6 |
Full active range of movement, good scapular control |
|
Return to Functional Activities |
|
| Driving |
|
| Swimming |
|
| Golf |
|
| Racquet Sports/Repeated Overhead Activities |
|
| Lifting |
|
| Work |
|
Success of Surgery, Risks & Complications
An Arthroscopic Subacromial Decompression and Excision of Calcific Deposit is usually a very successful procedure but, because the surgery is only aimed at removing the spur of bone that has been impinging on the Supraspinatus Tendon, it usually takes between 3 – 6 months for the Tendonitis to settle and for the Shoulder to return to normal. For a standard Arthroscopic Subacromial Decompression>95% of patients’ will be happy with their shoulders after 6 months.
There are always risks and complications associated with any operation.
- Anaesthetic - The risks of having a General Anaesthetic and an Interscalaene Nerve Block are very low, but will always need to be assessed on an individual basis by an Anaesthetist. Suffice it to say, that whilst a Shoulder Operation can in no way be considered a ‘life-saving’ procedure, an Anaesthetist would not consider undertaking an anaesthetic if they had any concerns that an undue risk was being taken.
- Infection – Infection following arthroscopic surgery is rare < 0.2%
- Neurovascular Injury – Damage tosignificant neurovascular structures during arthroscopic shoulder surgery is rare < 0.2%
- CRPS Type 1 – A Chronic Pain Syndrome following arthroscopic shoulder surgery is rare < 0.2%
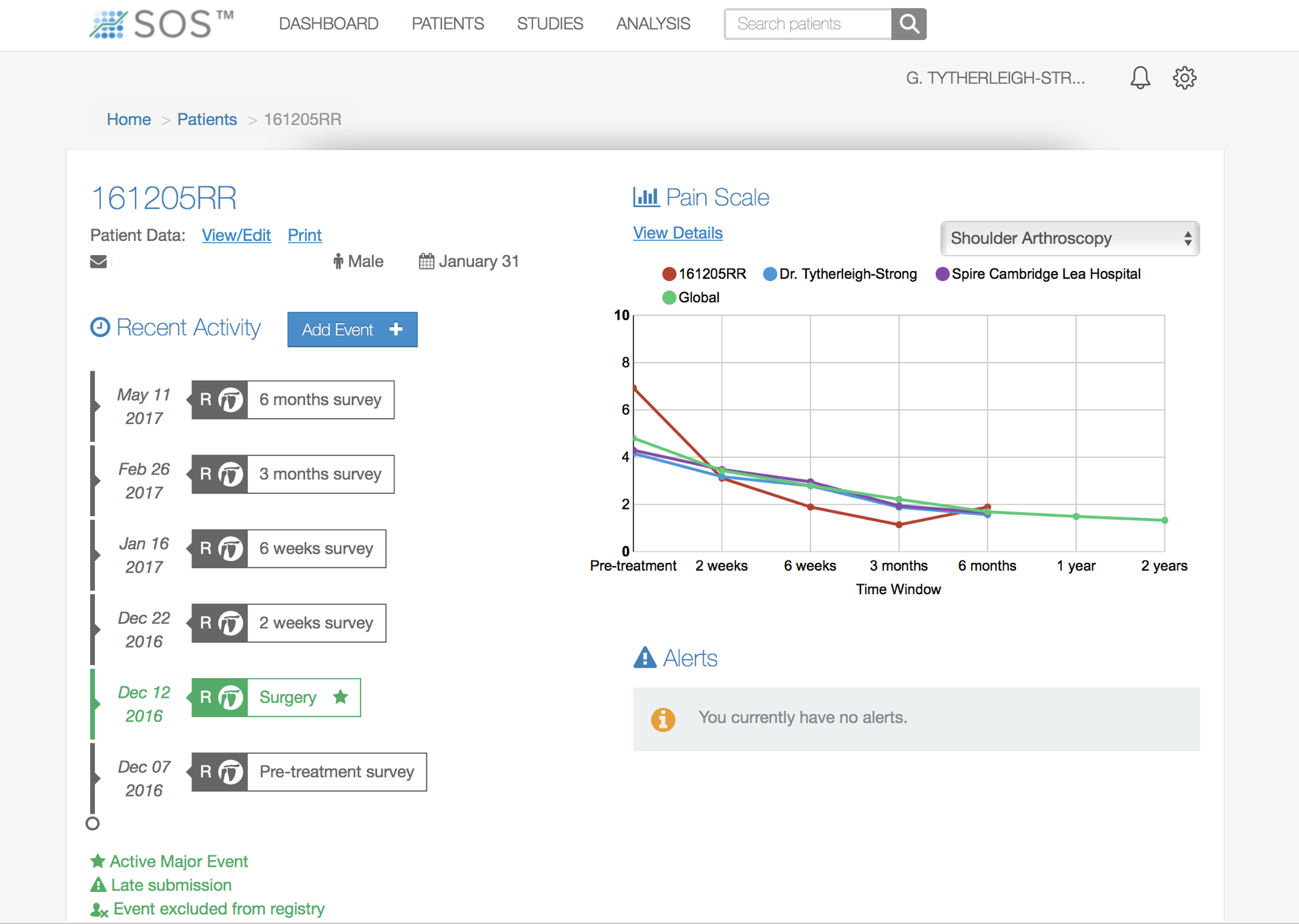
Outcome Measures
Assessing patient outcomes following surgery, using validated scoring systems, is a very important and useful exercise.
Management of Acute Calcific Tendonitis
- An Acute Calcific Tendonitis usually occurs so rapidly and is so painful that urgent treatment is required
- Subacromial Cortisone Injection –
- In some cases of an Acute Calcific Tendonitis a Cortisone injection can rapidly alleviate the pain and settle the symptoms down. Often within a few days
- Cortisone is a corticosteroid that is naturally produced by the body’s Adrenal Gland. Injectable Cortisone is synthetically produced and has a very powerful ant-inflammatory action. When injected into the Subacromial space it has the potential of settling the severe inflammation associated with an Acute Calcific Tendonitis, allowing the patient to undertake their rehabilitation exercises.
- A Subacromial Cortisone can be easily administered in the Out-Patient Clinic. It is a quick and relatively painless procedure. Afterwards patients can continue with their normal day-to-day activities. Occasionally patients can feel a bit of soreness around their shoulder later that day, but this usually passes fairly quickly.
- The Cortisone works in the background and there is no specific requirement to particularly rest the shoulder or to do extra exercises. The immediate benefits of a Cortisone injection should be felt within a few days. However, the full benefits of a Cortisone injection may take a month.
- Infections can occur after any type of injection but are extremely rare (1 in 15,000). If someone feels that they are developing an infection within 48 hours of a Cortisone injection they should seek advice from their Family Practitioner.
- Surgery for Acute Calcific Tendonitis – If the severe pain associated with an Acute Calcific Tendonitis does not begin to improve at all, within a few days, surgery is the only option to gain a rapid benefit.
Arthroscopic Excision of an Acute Calcific Tendonitis +/- Subacromial Decompression
The best operation for someone with an Acute Calcific Tendonitis, that has not responded to a Cortisone injection, is an Arthroscopic Excision of the Acute Calcific deposit. This is an operation where an Arthroscopic camera is positioned inside the Subacromial Space and, by using specialized instruments, the Calcific Deposit is removed from within the tendon.
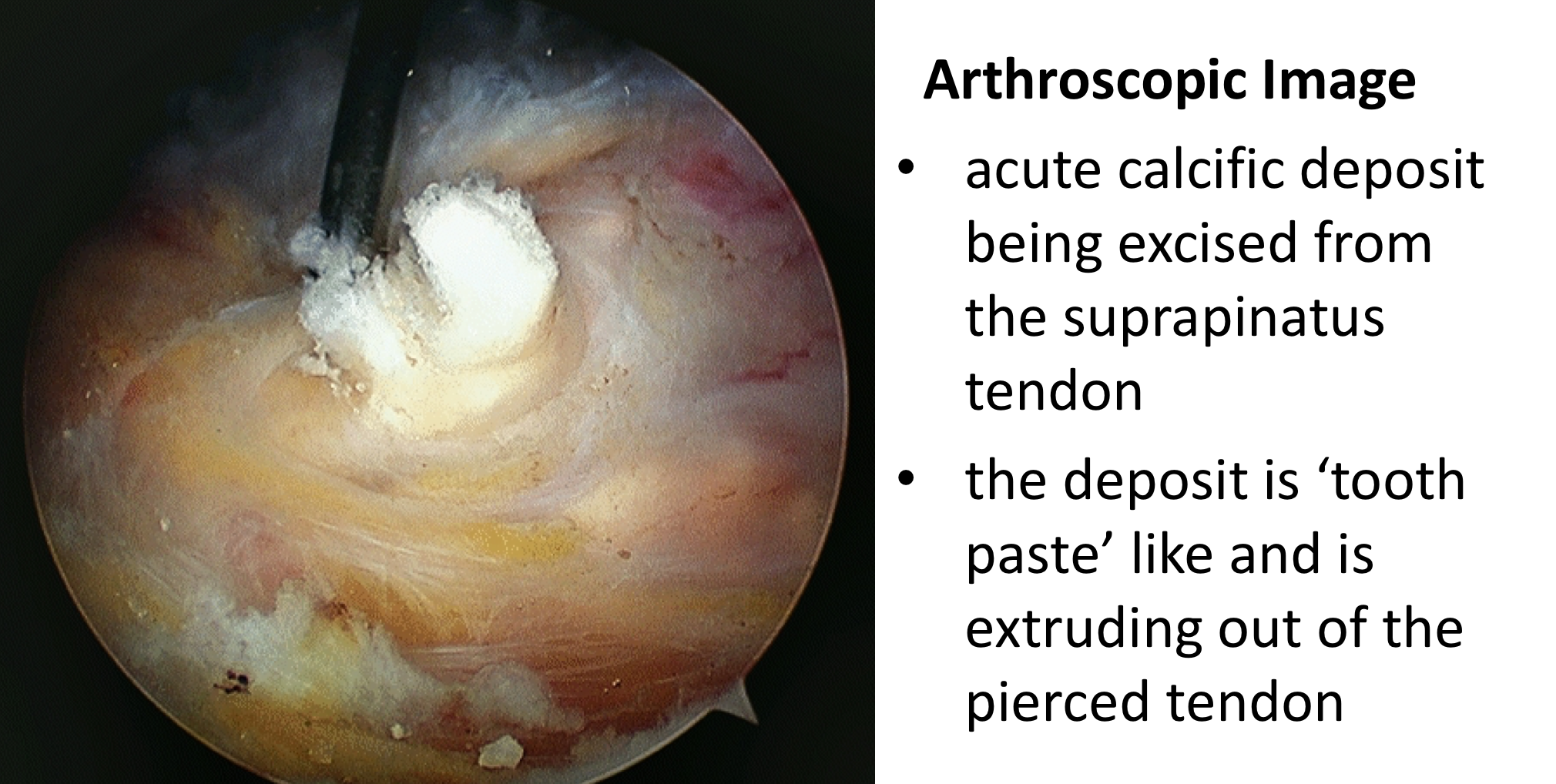
In an Acute Calcific Tendonitis the symptoms occur at such an early stage that the deposit is still usually in a fluid / ‘tooth-paste like’ stage. As a result, just opening up the tendon or multiple needle punctures are enough to allow it to fully extrude under pressure. The tendon does not need to be repaired and a decision can be made as to whether a Subacromial Decompression may help with recovery.
An Arthroscopic Excision of an Calcific deposit can usually be done as a Day Case procedure and the patient’s shoulder does not need to be immobilized for anytime afterwards, unless an additional rotator cuff repair has been undertaken. The surgery aims to extract the rapidly expanding deposit. It usually results in a major relief of the severe pain, but it can take between 3 – 6 months to gain the full benefits of the procedure. It has a high success rate with around 95% of patients being happy with the result 6 months after their operation. My routine Arthroscopic Excision of an Acute Calcific Deposit Procedure is described below,
Watch a video of an Arthroscopic Excision of an Acute Calcific Tendonitis…(Research & Education – Video – Acute Calcific Tendonitis)
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
- A posterior and a single lateral portal are used for to view the Gleno-Humeral Joint (Shoulder Joint) and Subacromial spaces
- The Glenohumeral Joint is initially assessed to look for any other problems that might be associated with a Supraspinatus Tendonitis and, in particular, the Rotator Cuff and the Long Head of Biceps
- The Subacromial Space is then entered and the undersurface of the Acromion identified.
- A lateral portal is then created
- The Supraspinatus Tendon is then inspected and the area of the Calcific Deposit identified
- Either using a needle or a punch the tendon is pierced and the Calcific Deposit seen to extrude, rather like ‘tooth-paste’ coming out of a tube
- After removal of the Calcific Deposit the undersurface of the anterior acromion is assessed and, if there is a significant prominence, a decompression performed
- The Subacromial Space is then washed out and the wounds closed with sub-cuticular sutures
After the Surgery
Post-Operative Care
Following an Arthroscopic Excision of an Acute Calcific Deposit the patient is usually able to go home on the same day as their surgery. I would see the patient after the surgery to discuss how the procedure has gone and arrange for further Follow-Up. The patient will be seen by the In-Patient Physiotherapy team, who will instruct them on the initial Rehabilitation Protocol for their shoulder. Further Out-Patient physiotherapy will then be organised.
Find out more about Physiotherapy following an ASD….
I would usually review patients in the clinic 1 month and 3 months after their procedure to assess their progress and recovery.
Rehabilitation Protocol
Immediately after the surgery, when the patient has woken up from their general anaesthetic, their shoulder and arm will be numb from the interscalaene nerve block. This will usually last for 18 – 24 hours after the surgery. For this period, we advise patients to keep their arm in a sling, purely for protection. After the nerve block has worn off the arm can begin to be taken out of the sling. I encourage patients to wean themselves off of using the sling as quickly as possible, within the limits of discomfort.
My standard rehabilitation protocol is outlined below for a standard procedure. The information and time to recovery are a general estimation and may vary from person to person.
|
Post op |
|
| Immediate |
|
| Day 1-3
Weeks |
|
| 3-6 Weeks |
|
|
Milestones |
|
|
Week 3 |
Full passive range of movement |
|
Week 6 |
Full active range of movement, good scapular control |
|
Return to Functional Activities |
|
| Driving |
|
| Swimming |
|
| Golf |
|
| Racquet Sports/Repeated Overhead Activities |
|
| Lifting |
|
| Work |
|
Success of Surgery, Risks & Complications
An Arthroscopic Subacromial Excision of an Acute Calcific Deposit is usually a very successful procedure but, because the shoulder and tendon have been very inflamed it can take between 3 – 6 months for the Shoulder to return to normal. For a standard Arthroscopic Subacromial Decompression>95% of patients’ will be happy with their shoulders after 6 months.
There are always risks and complications associated with any operation.
- Anaesthetic - The risks of having a General Anaesthetic and an Interscalaene Nerve Block are very low, but will always need to be assessed on an individual basis by an Anaesthetist. Suffice it to say, that whilst a Shoulder Operation can in no way be considered a ‘life-saving’ procedure, an Anaesthetist would not consider undertaking an anaesthetic if they had any concerns that an undue risk was being taken.
- Infection – Infection following arthroscopic surgery is rare < 0.2%
- Neurovascular Injury – Damage tosignificant neurovascular structures during arthroscopic shoulder surgery is rare < 0.2%
- CRPS Type 1 – A Chronic Pain Syndrome following arthroscopic shoulder surgery is rare < 0.2%
Outcome Measures
Assessing patient outcomes following surgery, using validated scoring systems, is a very important and useful exercise.
find out more about outcome measures and the SOS system…