What is Shoulder Instability
Shoulder Instability is a general term for any type of problem that results in the Humeral Head (Ball) not being centred firmly into the glenoid (Socket). It can range from,
-
Dislocation - complete dislocation of the head
-
Subluxation - an incomplete dislocation where the Humeral Head slips to the edge of the Glenoid socket and almost dislocates, but is ‘caught’ just before this happens.
-
Micro-Instability – A situation where the Humeral Head does not feel completely stable in certain positions of movement.
Shoulder Stabilisers
The shoulder is the most mobile joint in the body with a relatively small socket (gelnoid) and large head (humeral head). This configuration means that it is potentially unstable and it is the most frequently dislocated joint in the body. Fortunately, this still occurs relatively rarely and is because there are a number of mechanisms that help to keep it in joint. These are divided into 2 groups,
-
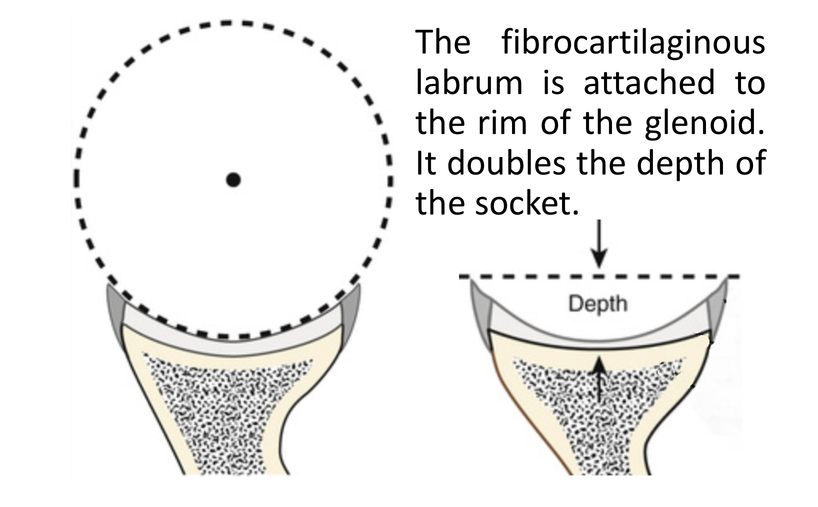
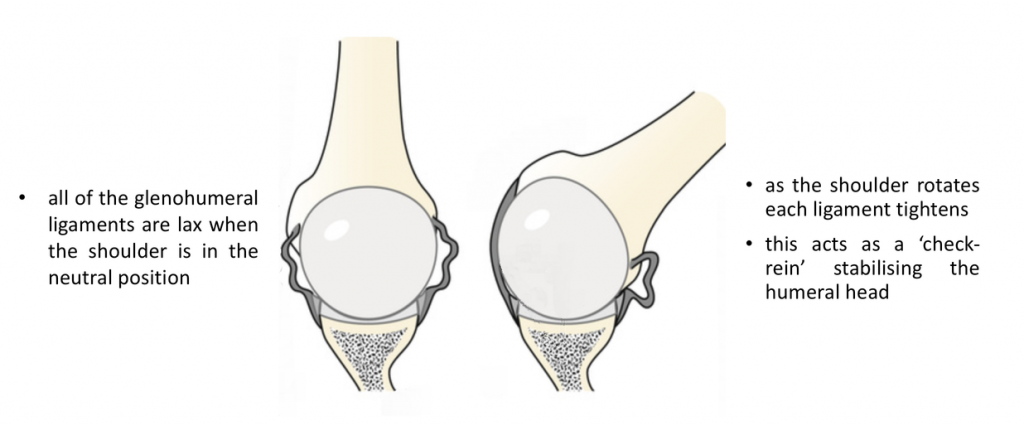
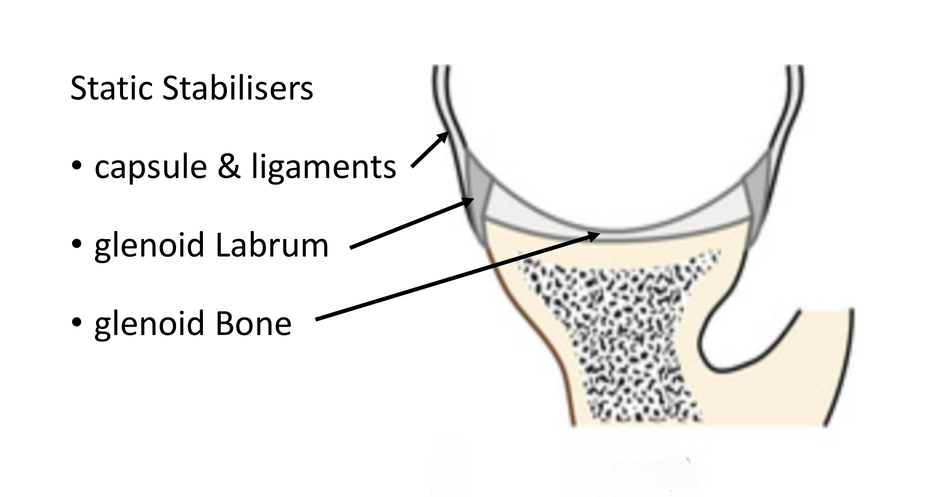
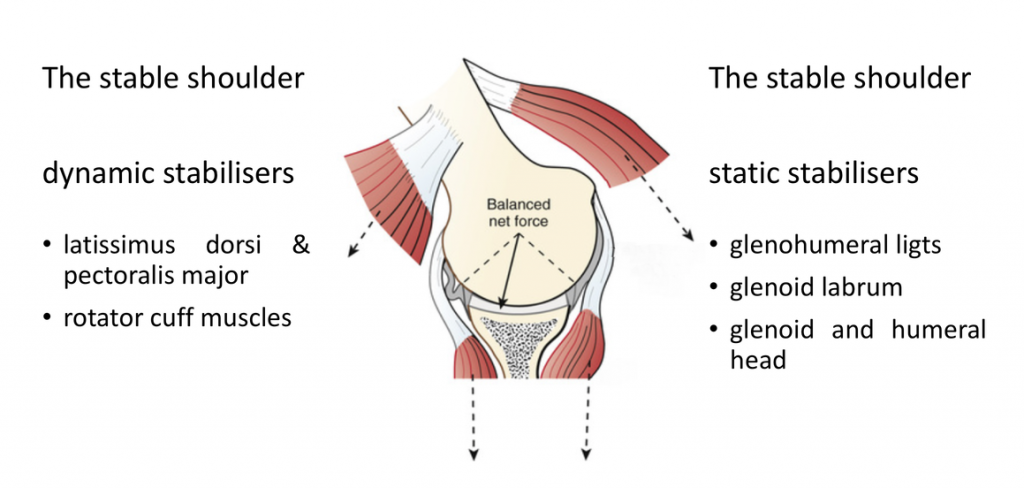
Static Stabilisers – these are the socket (glenoid) with its convex shape, the glenoid labrum (that deepens the socket) and the ligaments that connect the ball to the socket.
-
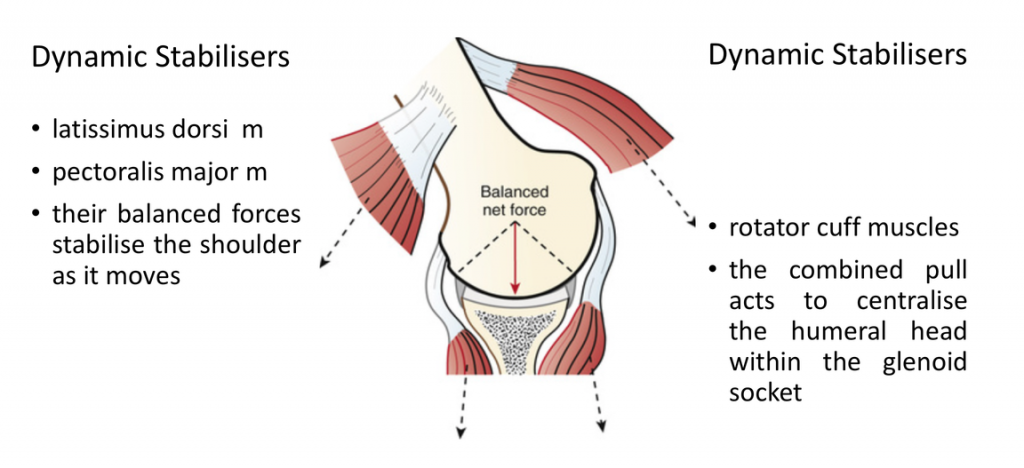
Dynamic Stabilisers – these are the multiple groups of muscles that surround the shoulder girdle and work in a complex rhythm to move the shoulder whilst keeping it in joint.
Types of Dislocations
This section covers shoulder dislocations. Labral Tears/SLAP tears cause a specific type of instability which is covered in its own section.
When the shoulder dislocates or subluxes it will be due to an injury or failure of either the dynamic or static stabilisers or both. There are 3 ways in which shoulder stability fails,
-
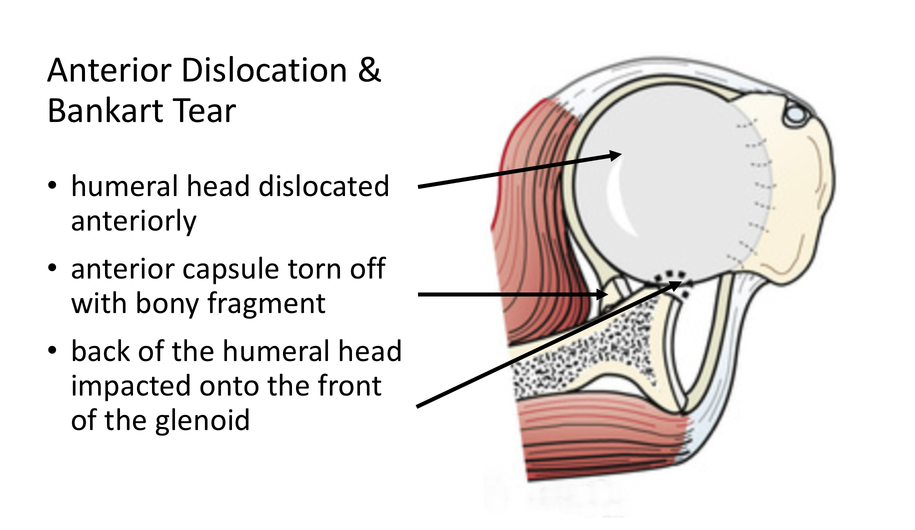
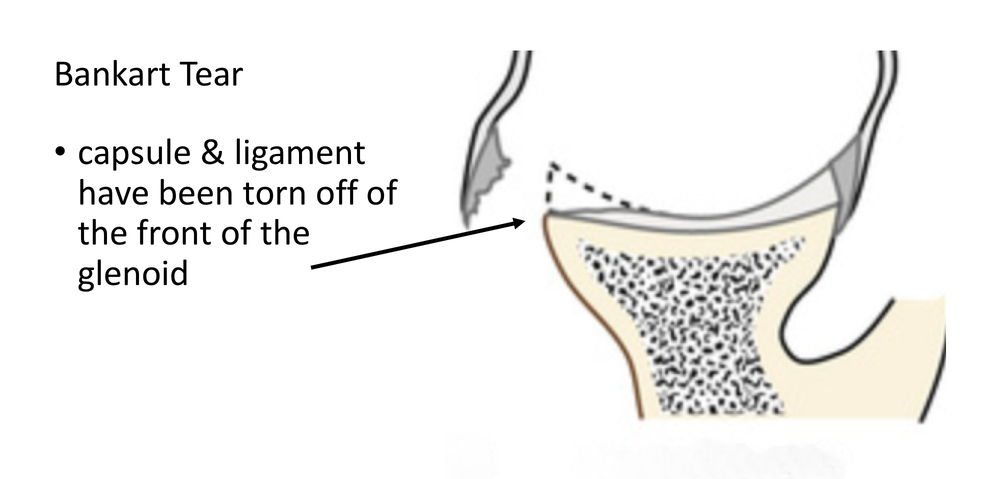
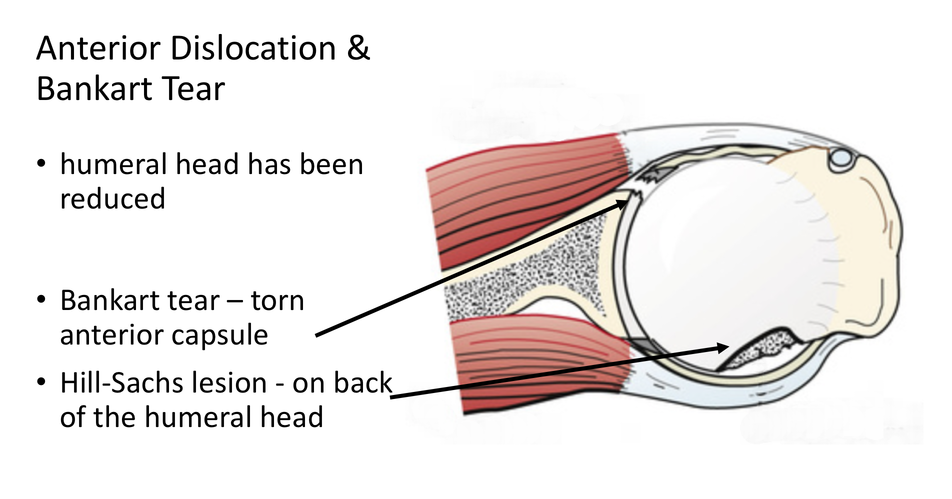
Traumatic Injury – this is the commonest cause for shoulder dislocations. Usually the patient sustains a significant injury where they fall forwards with the arm elevated, the elbow bent and the hand facing forwards (being tackled playing rugby, falling skiing or from a horse etc). The humeral head is then forced forward tearing the ligaments at the front of the shoulder and sometimes damaging the bone at the front of the socket and the back of the head. Patients usually are unable to relocate their shoulder and need this to be done at a medical centre. Occasionally the labrum and ligaments can be damaged by repeated smaller injuries to the shoulder until they eventually fail.
-
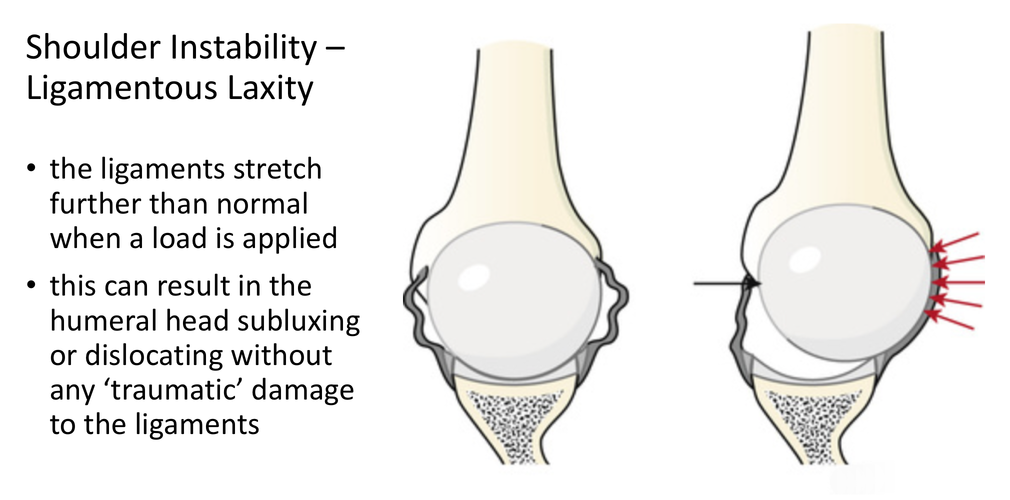
Ligamentous Laxity - some peoples’ tissues are more lax/stretchy than others. This tends to occur more often in females than males and in younger people. In certain cases the ligaments around the shoulder are so lax that they are unable to completely restrain the ball within the socket. This can result in subluxation or dislocation of the shoulder without a significant injury. When this does occur the ball can dislocate in any direction leading to mult-directional instability.
-
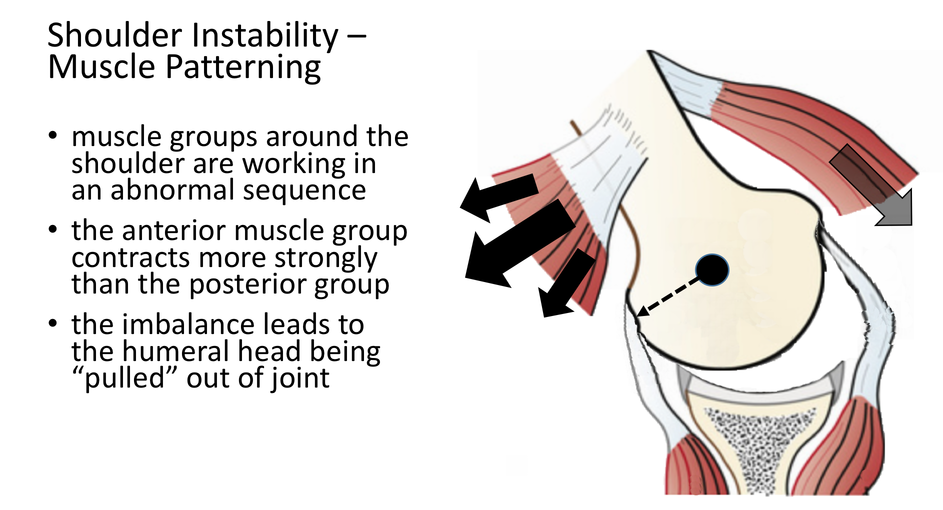
Muscle Patterning Disorder – occasionally the complex sequence in which the groups of muscles work to stabilise the ball into the socket as the shoulder moves become disrupted. In this situation muscles that should be contracting, relax or aren’t strong enough whilst other muscles that should be relaxing, contract. This can result in the shoulder being ‘pulled’ out of the socket by this muscle imbalance. The static stabilisers of the shoulder are often completely intact.
In some cases of shoulder instability more than one of the above problems can be going on at the same time.