
Scapula Anatomy
- Scapula
- The Scapula, or shoulder blade, is a triangular shaped bone that lies over the upper part of the back
- It is not directly attached to the axial skeleton, apart from the acromioclavicular joint (ACJ) and the clavicle, and is held in position by a complex arrangement of muscle attachments that come off of the chest wall and spinal column
- It forms the socket part, glenoid, of the Glenohumeral Joint (GHJ)
- Its function is to provide a ‘stable’ base for the GHJ to function, whilst also contributing some additional over 30% of the movement to the shoulder as it glides over the chest wall
Bones
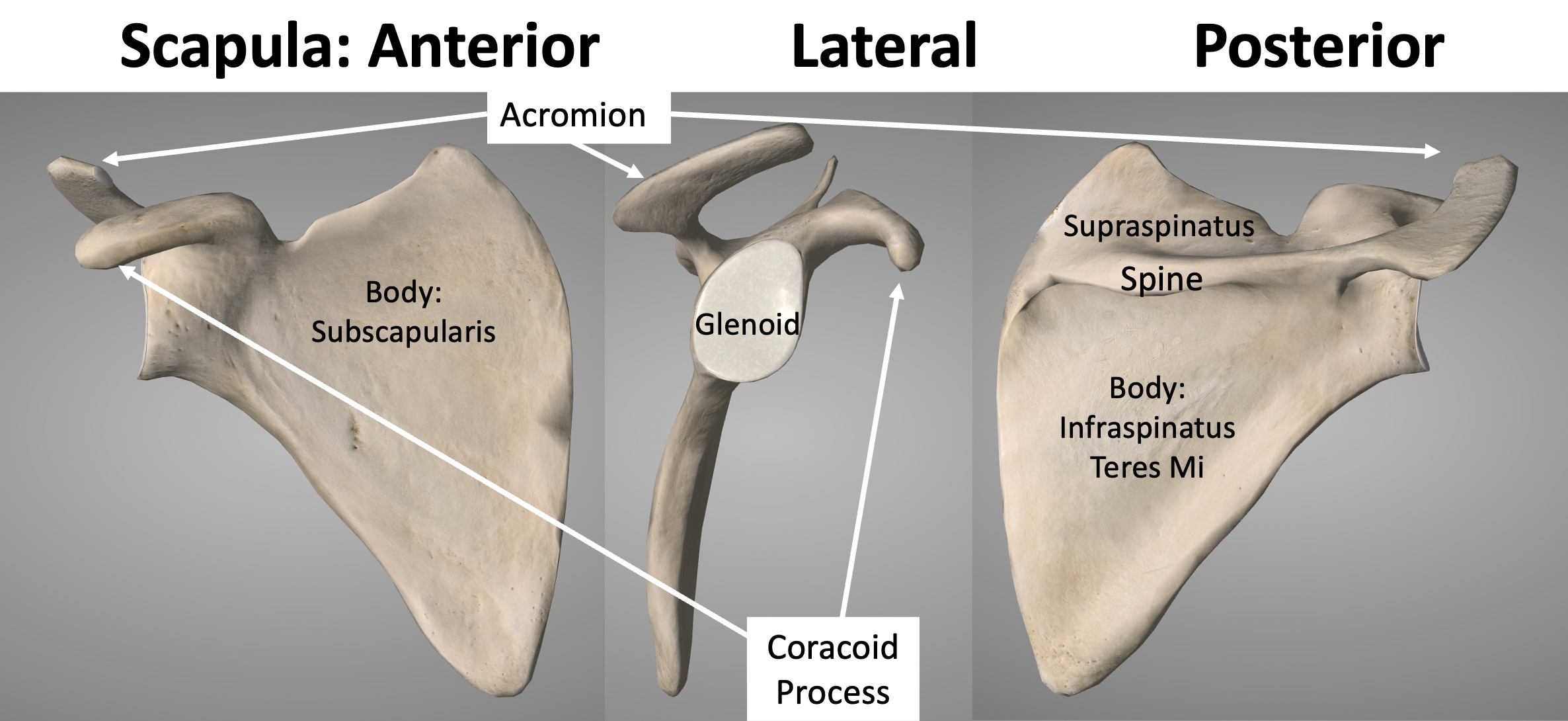
- The scapula is a single triangular shape bone but has a number of different parts that each play a key role in its function
- Glenoid – this forms the ‘socket’ part of the Glenohumeral Joint
- the glenoid labrum deepens the socket and the capsule and glenohumeral ligaments attach circumferentially
- the long head of biceps & the long head of triceps take their origin from the top and the bottom of the bone
- Body – the triangular shaped body is formed by a strong surrounding outer rim of bone, whilst the central bone is relatively thin
- the various muscles that are involved in both stabilising and moving the scapula insert circumferentially around the rim
- all of the rotator cuff muscles, that move and stabilise the GHJ, originate from the central bone
- Acromion & Spine
- the spine is a thickened ridge of bone over the back of the scapula which blends into the acromion
- they provide the origin and insertion of the Trapezius and Deltoid muscles which are important in both stabilising and moving the scapula and the GHJ
- the anterior, lateral edge of the acromion forms part of the Acromioclavicular Joint (ACJ). This is the only mechanical connection between the scapula and the axial skeleton
- Coracoid Process
- the coracoid process is a hook shaped bone on the front of the scapula
- the Coracocavicular ligaments (CC), which play a very important role in stabilising the ACJ attach to the top of the coracoid
- the Conjoint Tendon, formed from the short head of biceps and caoracobrachailis originate from the tip of the coracoid
- Glenoid – this forms the ‘socket’ part of the Glenohumeral Joint
Muscles
- the scapula is completely surrounded and covered by muscles, which can be divided into 3 groups
- Rotator Cuff Muscles
- the 4 Rotator Cuff muscles all take their origin off of the anterior and posterior surfaces of the Body of the Scapula
- they are directly involved in both stabilising the humeral head onto the glenoid and moving the GHJ
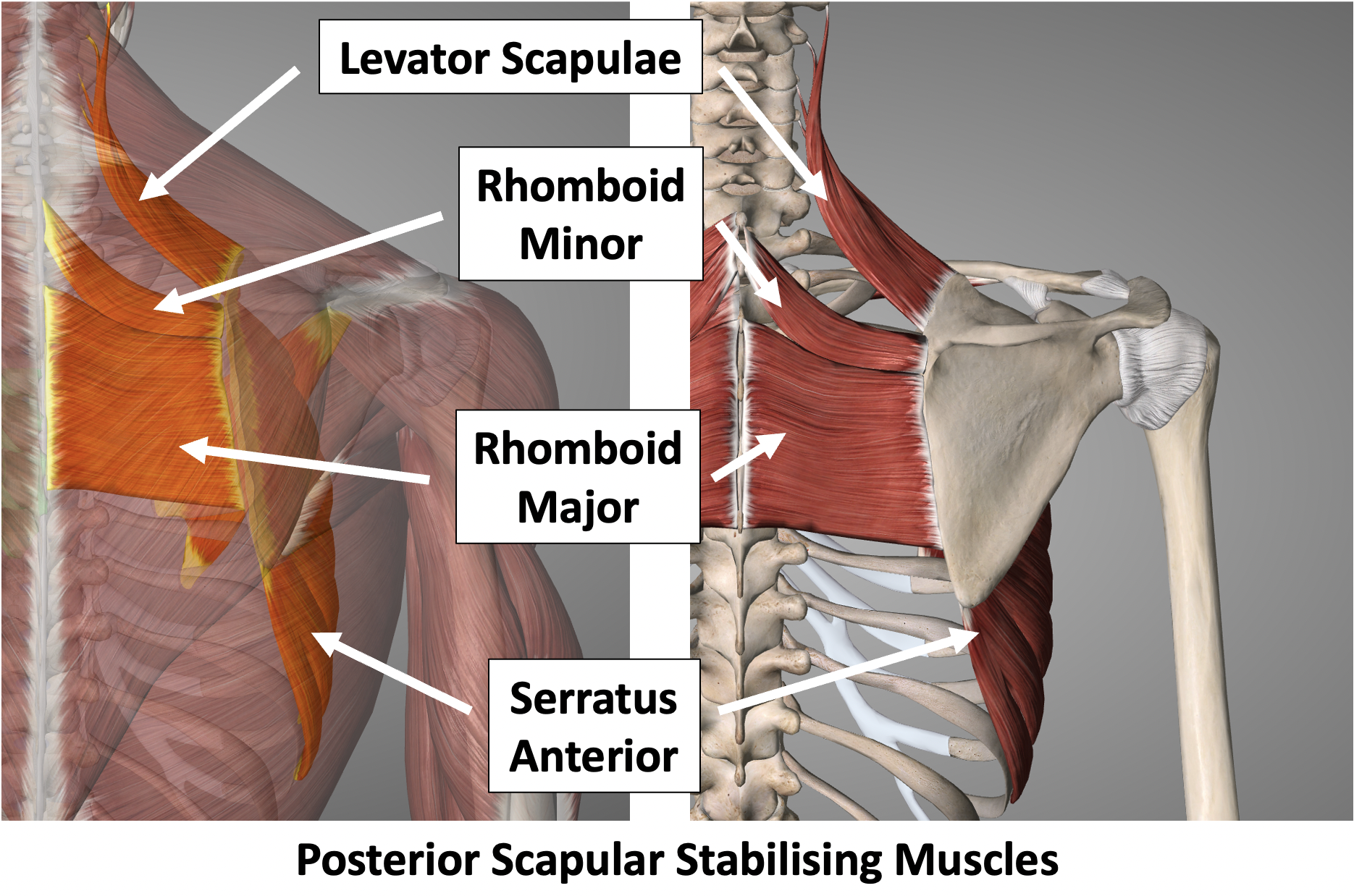
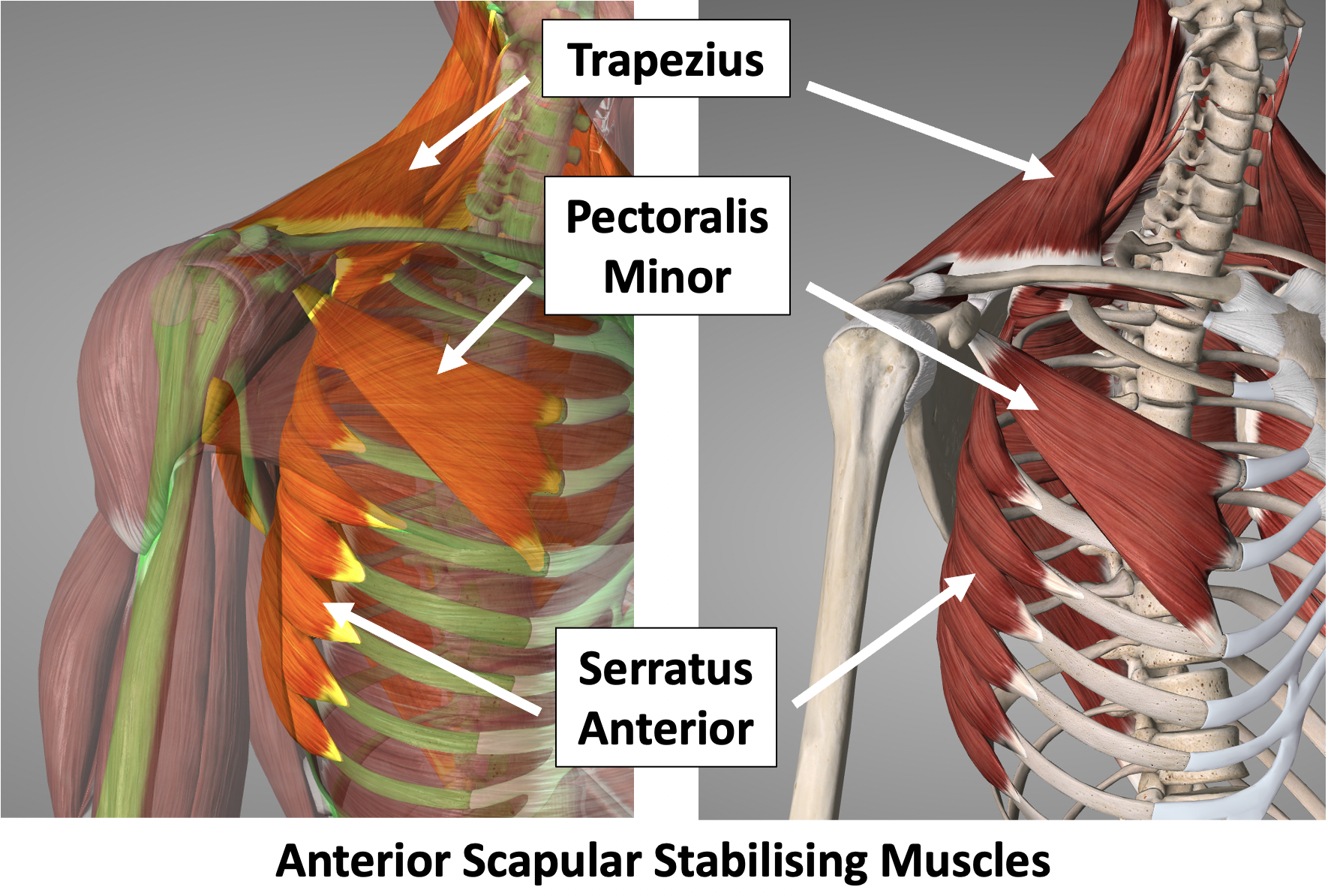
- Scapular Stabilising Muscles
- muscles that originate from the spinal column and the chest wall and insert circumferentially along the edge of the scapula
- these muscles work as a co-ordinated unit and serve 2 functions
- they firmly stabilise and position the scapula onto the chest wall to provide a stable ‘base’ for the GHJ to function
- they are also able to allow the scapula to move position on the chest wall to aid overall shoulder movement – this is sometimes referred to as the ‘Scapulo-Thoracic’ joint
- Upper Arm Muscles
- these muscles provide strength and movement to the upper arm and elbow
- Rotator Cuff Muscles
Scapula Function
The Scapula performs a number of functions which all play an important role in the function and movement of the shoulder and elbow
- Glenohumeral Movement (shoulder joint)
- The Glenoid Fossa is part of the Scapula and forms the ‘socket’ part of the Glenohumeral joint
- The Scapula his held in a stable position onto the chest wall which allows, the Humeral Head, the ‘ball’ part’ of the Glenohumeral joint, to move freely
- The 4 Rotator Cuff muscles and their tendons, which help to both stabilise and move the Humeral Head, take their origin from the blade of the Scapula and pass over the Glenohumeral joint and attach onto the Humerus
- Movement at the Glenohumeral joint accounts for about 67% of the total shoulder movement
- Scapulo-Thoracic Movement
- Whilst the Glenoid Fossa provides a stable platform for the Glenohumeral joint, the whole of the scapula can move over the posterior chest wall providing an additional 33% to the overall movement of the shoulder
- The stabilising muscles originating from the vertebral column and ribcage that attach around the periphery of the scapula work in a co-ordinated sequence to move the Scapula
- The attachment of the Clavicle to the Scapula at the Acromioclavicular Joint helps to ‘strut out’ the Scapula and helps to stabilise its movement
- Shoulder & Elbow Power and Movement
- The Biceps & Coracobrachialis muscles, that originate from the Coracoid process on the front of the Scapula provide power to Flex the shoulder and elbow
- The Long Head of the Triceps muscle, that originates from the inferior glenoid tubercle at the side of the Scapula
What is the Scapulothoracic Joint?
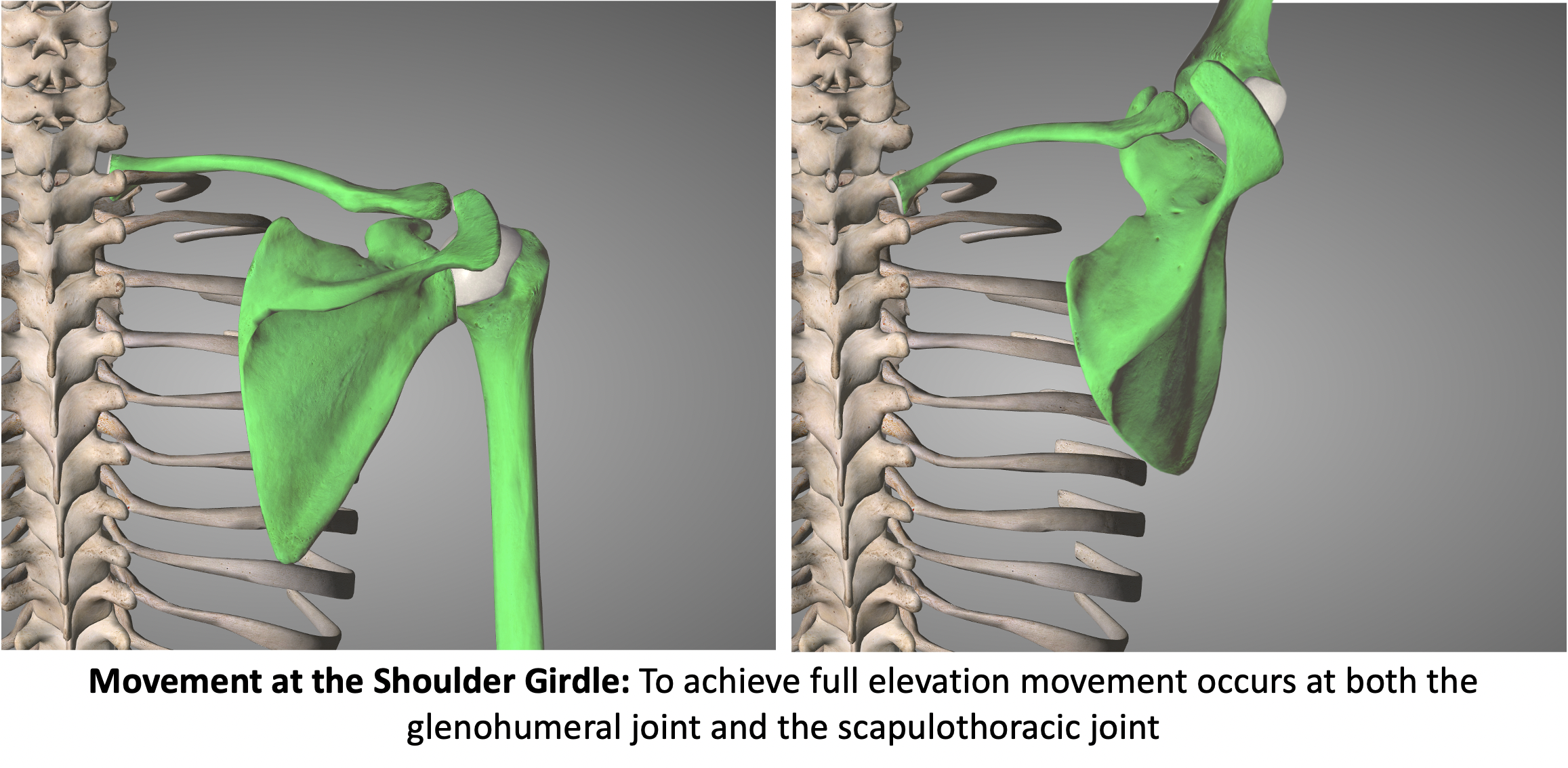
The Scapulothoracic Joint is not a true joint but describes the articulation of the scapula over the posterior chest wall. During normal shoulder movement, as well as the humeral head moving at the glenohumeral joint, the whole of the scapula rotates outwards and upwards on the chest wall, providing additional shoulder movement. The Scapulothoracic Joint is made up of a number of structural and muscular components that work in a co-ordinated sequence to move the scapula over the chest wall.
- Structural Components
- The scapula is connected through the ACJ, clavicle and SCJ to the sternum
- The whole of this construct moves in unison as the scapula travels over the posterior chest wall and are the components of the Scapulothoracic Joint
- Scapula
- ACJ (acromoiclavciular joint)
- Clavicle
- SCJ (sternoclavicular joint)
- Muscular Components
- The muscles involved in moving the Scapulothoracic joint take their origin from the vertebral column and chest wall and connect to the scapula and clavicle
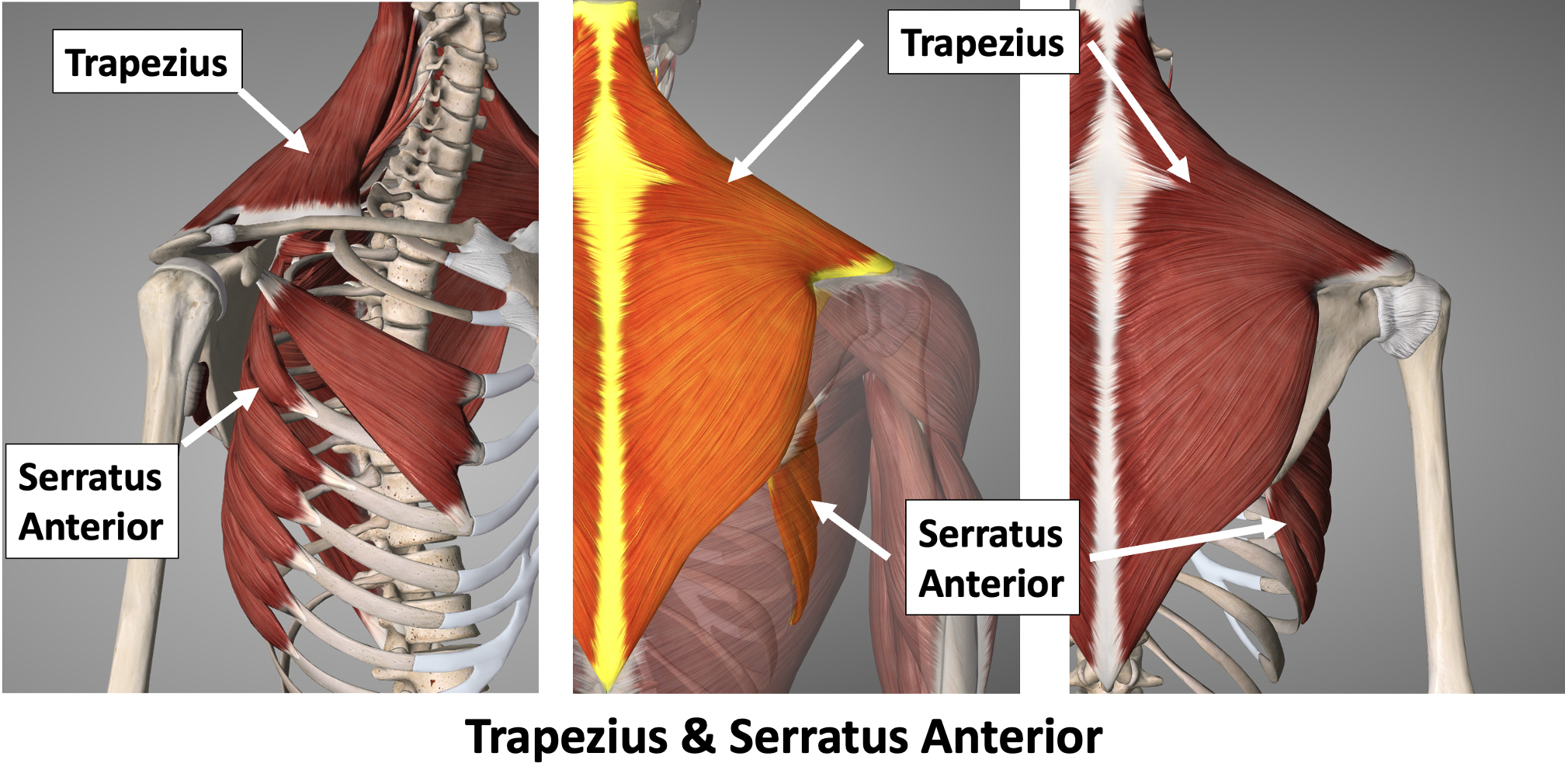
- Trapezius – vertebral column to scapula and clavicle
- Levator Scapulae, Rhomboid Major & Minor – vertebral column to scapula
- Serratus Anterior & Pectoralis Minor – chest wall to scapula
- The muscles involved in moving the Scapulothoracic joint take their origin from the vertebral column and chest wall and connect to the scapula and clavicle
- Co-Ordinated Movements
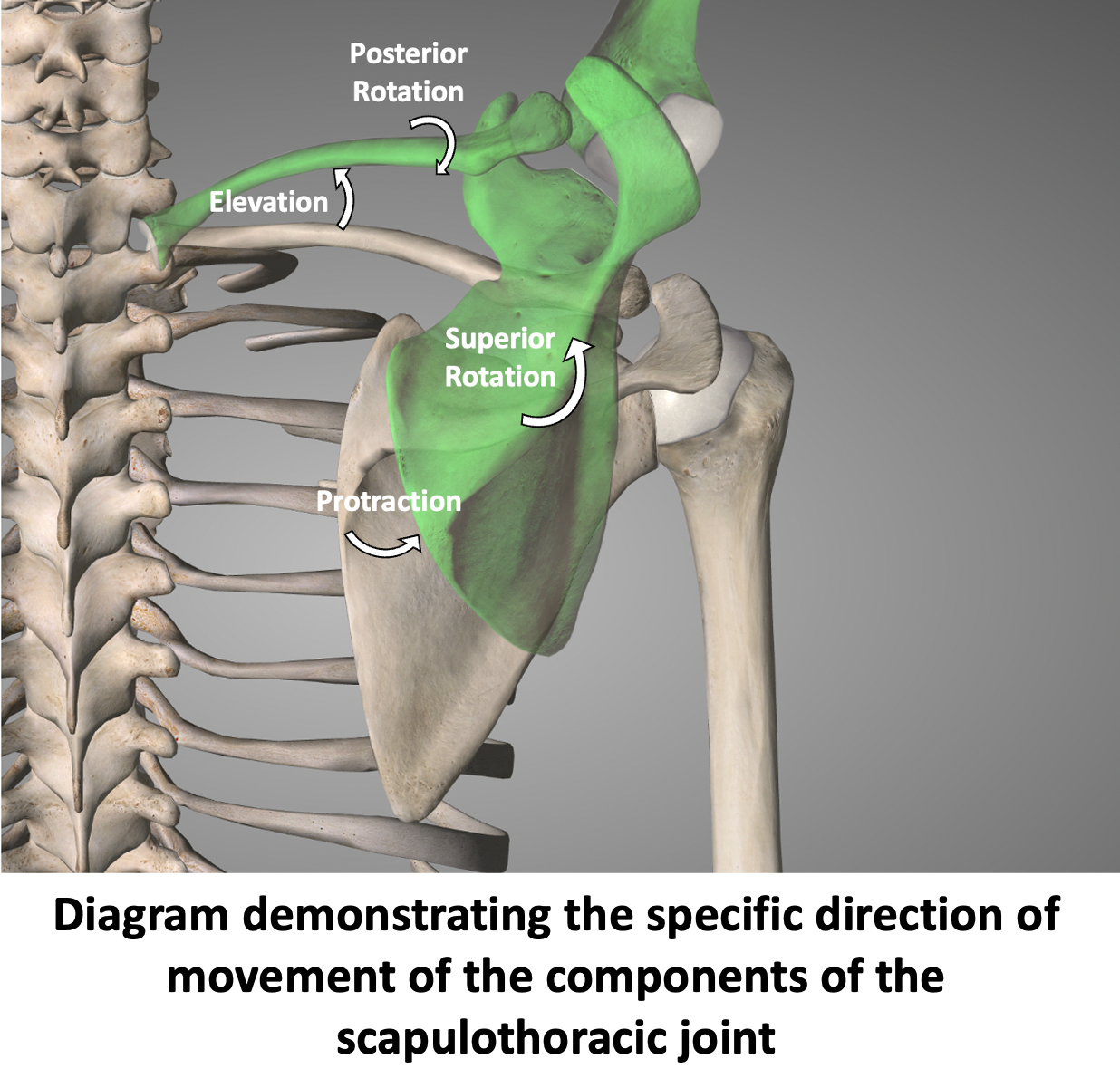
- Each of the Structural Components of the Scapulothoracic Joint move separately, but in a co-ordinated fashion, to move the Scapula on the chest wall
- SCJ – the joint elevates 400 and protracts 300
- ACJ – the joint elevates 50
- Clavicle – combined rotation at the SCJ & ACJ posteriorly rotates the clavicle 450
- Scapula – these combined movements can position the scapula, and so the glenohumeral joint, in 300 of protraction, 450 of elevation and 450 of posterior rotation
- Each of the Structural Components of the Scapulothoracic Joint move separately, but in a co-ordinated fashion, to move the Scapula on the chest wall
Scapula Problems
- Whilst there can be problems related to the function of the muscles, tendons & ligaments around the Glenohumeral Joint and with the various muscles that originate from the coracoid and the glenoid, the most specific problems that can affect the Scapula are with its stability and movement on the chest wall. This can be caused directly - as a result of a problem with the muscles stabilising the scapula, or indirectly - by the Scapula adapting its movement to try and compensate for a problem elsewhere in the shoulder girdle. There are 3 main types of Scapula Problems,
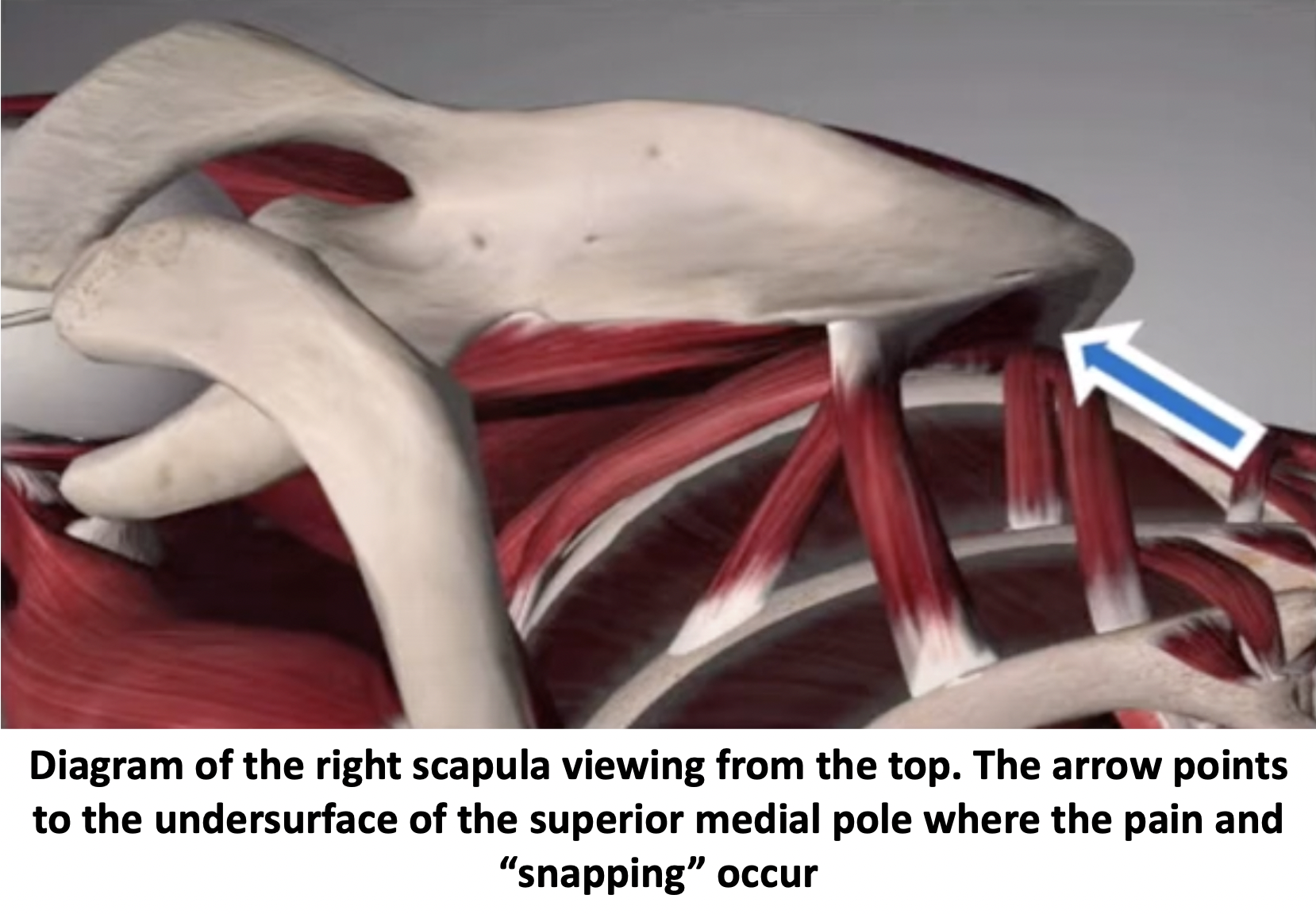
- Snapping Scapula Syndrome
- clicking and pain over the superior-medial (top of the inner edge) of the Scapula as it moves over the chest wall
- Scapula Dyskinesia
- a disturbance with the co-ordinate sequence of the stabilising muscles as they move the Scapula
- this can result in pain and weakness of the Scapula which can affect the stability and function of the Glenohumeral Joint
- the sequence disturbance can be caused by a problem with the Scapula and its stabilising muscles or by a problem elsewhere in the shoulder girdle resulting in the Scapula having to move abnormally to attempt to compensate
- Nerve Injury / Paralysis
- Two of the Scapula Stabilising muscles are each innervated by single nerves, which are both potentially susceptible to isolated injuries
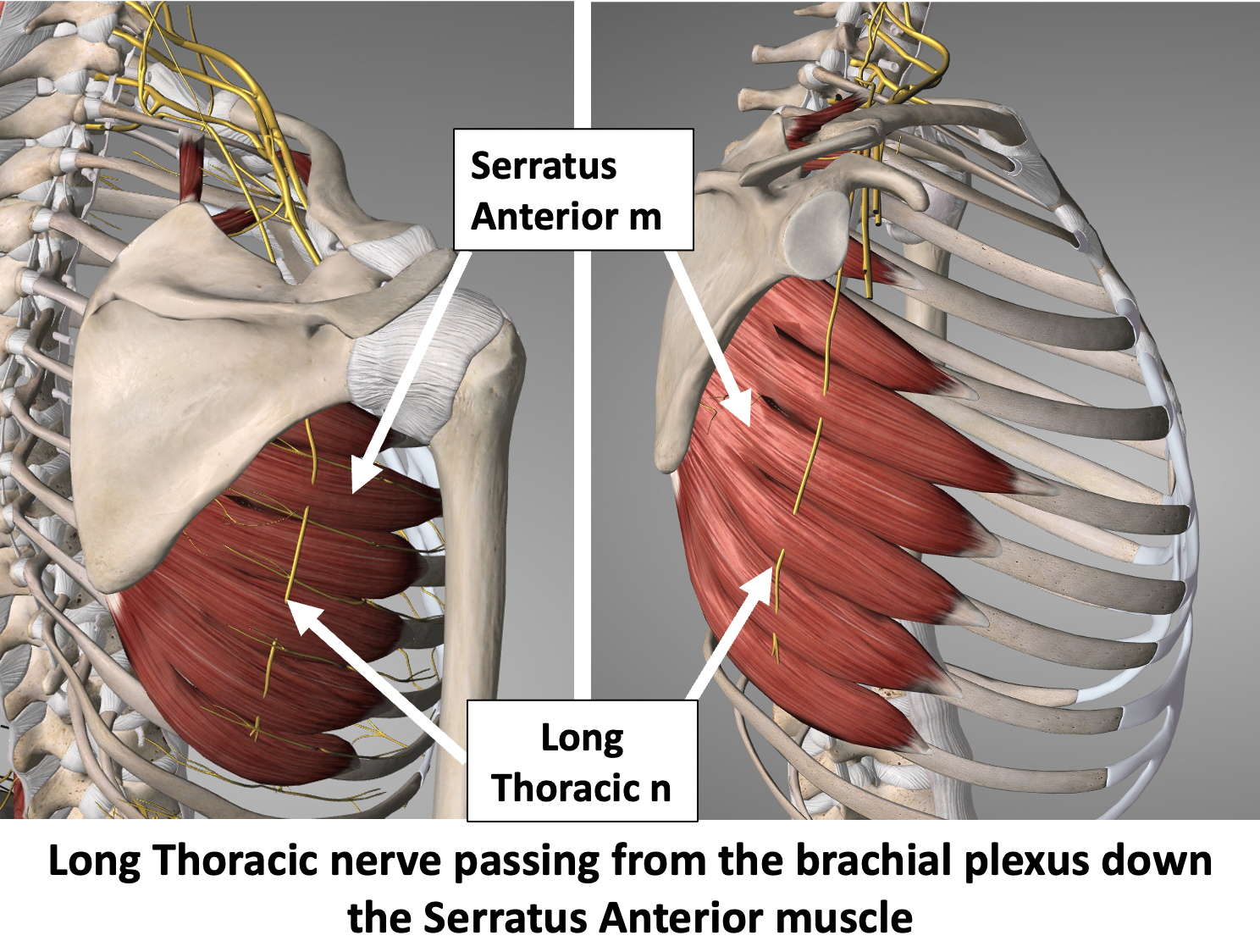
- Serratus Anterior – Long Thoracic Nerve
- Trapezius – Accessory Branch of the Eleventh Cranial Nerve
- Injury to either of these nerves can paralyse these muscles which can have a very significant effect on Scapula function
- Snapping Scapula Syndrome
Snapping Scapula Syndrome
Snapping Scapula Syndrome
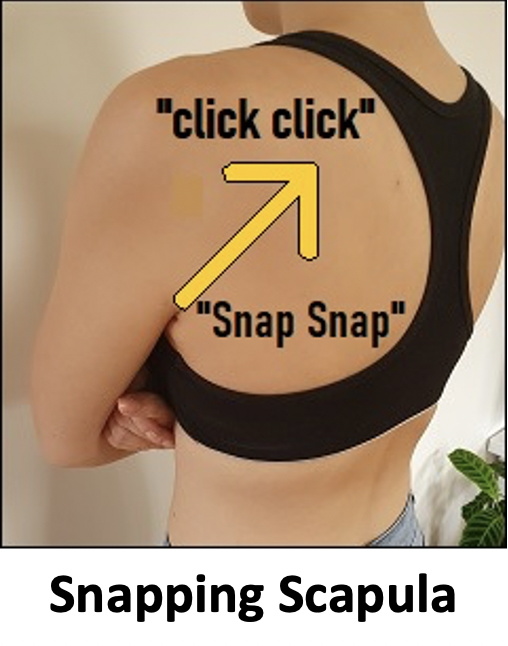
During normal shoulder girdle movement, the scapula moves over the chest wall. Whilst this movement is generally smooth in many people they can feel an element of “snapping”, “grinding”, ”clicking”, “crunching” of the top of the scapula over the chest at the base of the neck. This phenomenon is technically known as crepitus. In most people this is painless and, apart from the sensation and occasionally the sound, does not cause them any problems. It is entirely benign and does not need any specific treatment.
The snapping is due to the undersurface of the scapula rubbing/impinging on the muscles on the chest wall as the scapula protracts & retracts
- Snapping Scapula Syndrome (SSS)
- In certain situations, people can experience pain and a functional deficit associated with a snapping scapula
- Snapping Scapula Syndrome is the name given to this condition and there can be a number of different components / causes that can lead to this
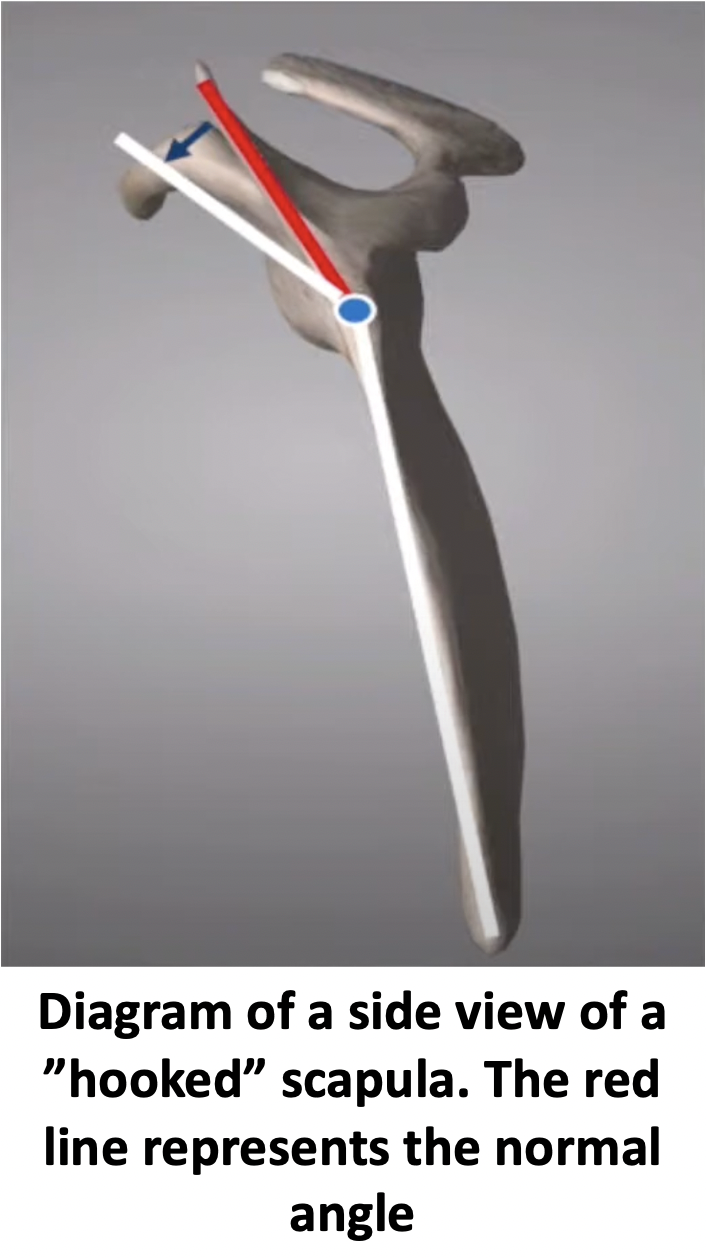
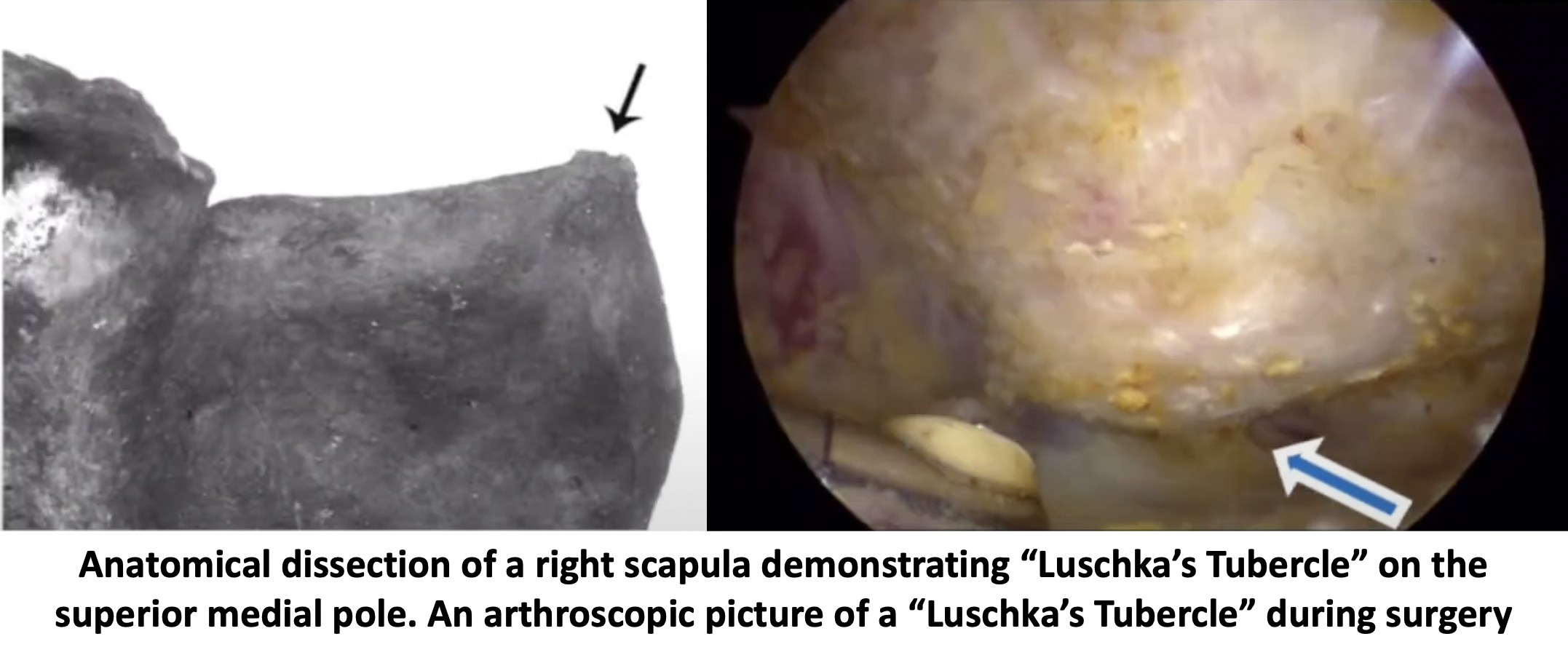
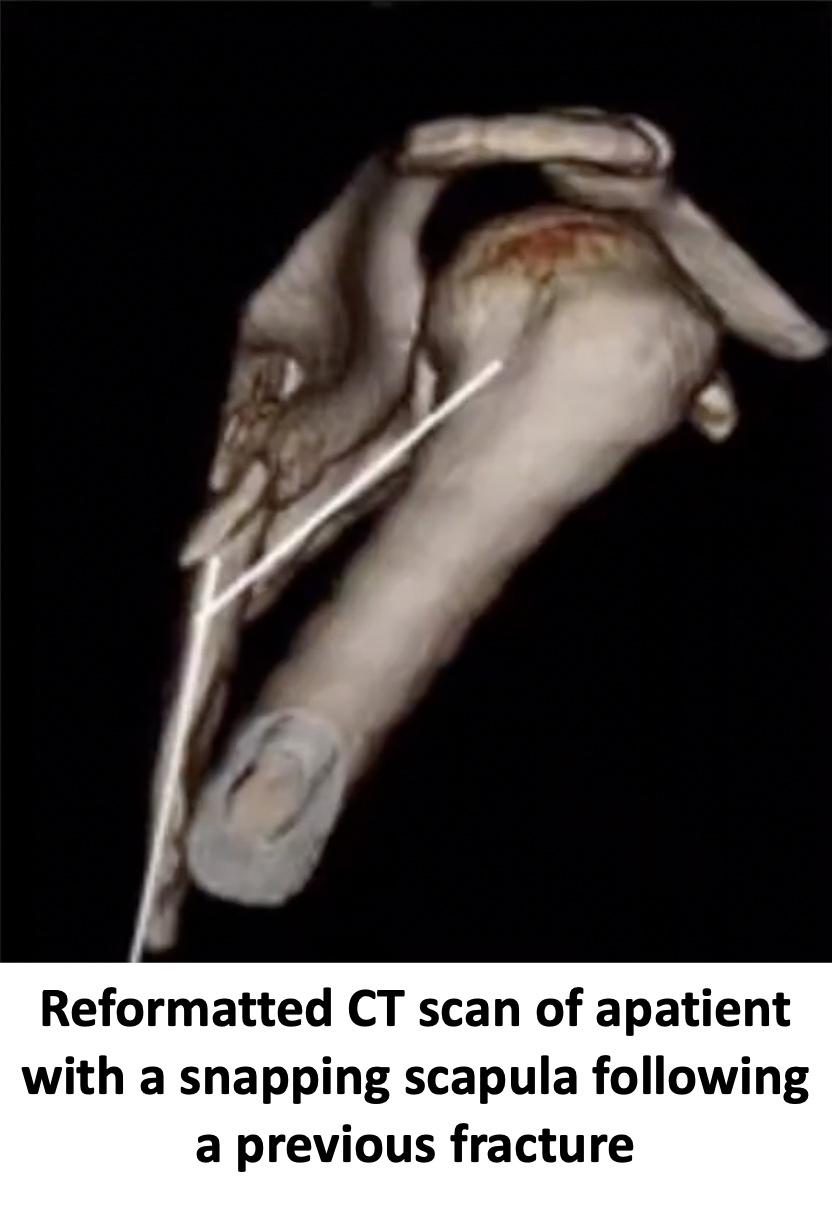
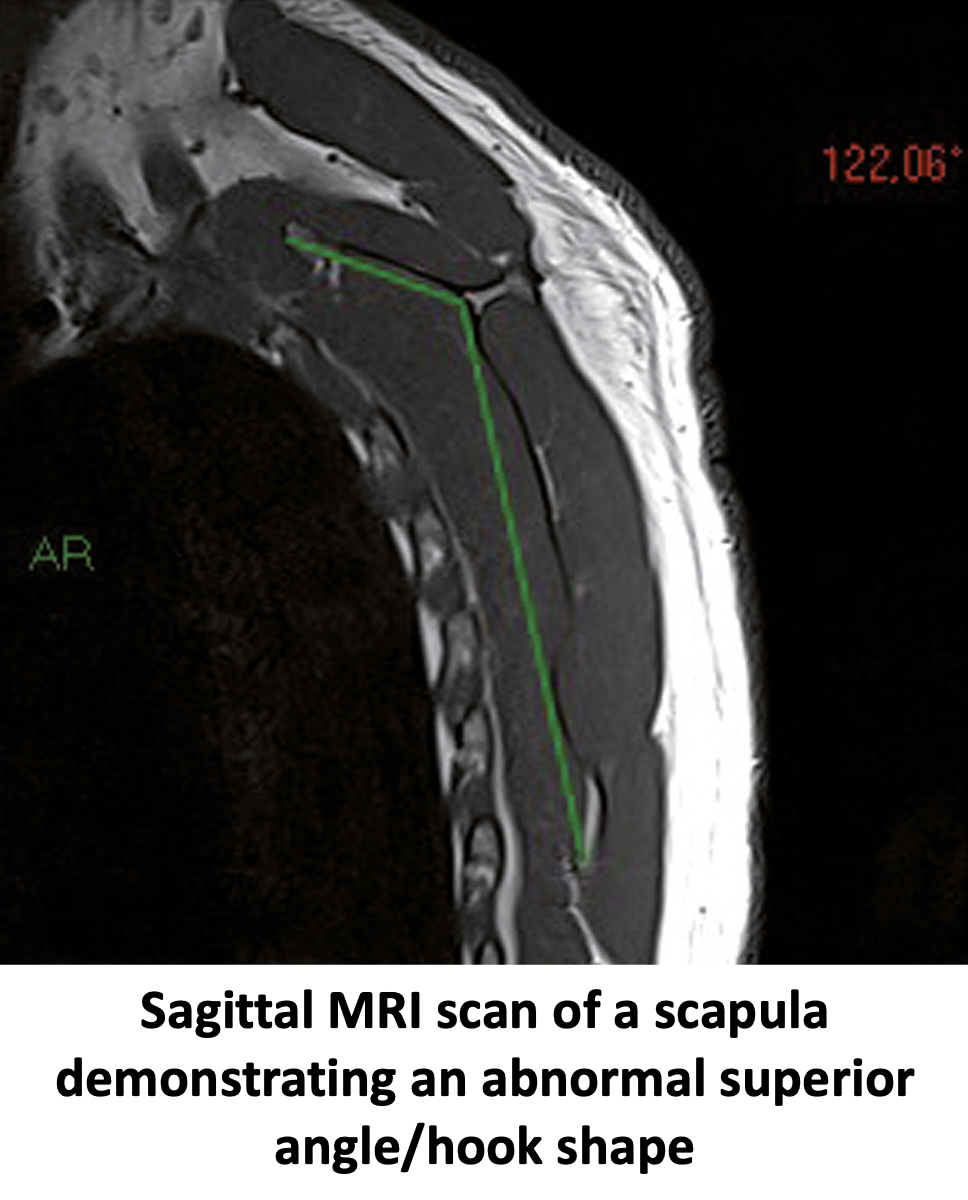
- Structural - structural causes may be due to a variation of the normal shape of the scapula. Some people have a more pronounced angle to the scapula and sometimes a “hook” shape to the superior medial pole of the scapula that can predispose them to developing crepitus and symptoms. This is known as the “Luschka’s Tubercle”. Sometimes an injury and fracture to the scapula may result in a distortion to its shape
- Occasionally bony growths (osteochondroma) or congenital abnormalities of the scapula may lead to SSS
- Functional / Dynamic – the muscles that stabilise and move the scapula have to work in a particular sequence. This sequence can be disturbed leading to abnormal movement of the scapula over the chest wall. This may be due to an overuse injury or a muscle tracking problem – Scapula Dyskinesia. This abnormal movement can result in SSS
- Neurogenic – occasionally the muscles around the scapula become painful which may be related to a nerve abnormality (neurogenic)
- Bursitis – there is a bursa that sits between the undersurface of the scapula and the chest wall. Its function is to help with the smooth movement between the two. When there is a disturbance of this movement the bursa can become inflamed causing a bursitis leading to pain
- What are the symptoms of Snapping Scapula Syndrome (SSS)?
- Onset of Symptoms
- In most cases SSS develops gradually over time without any specific precipitating cause
- However, occasionally, a specific incident or injury may lead to the onset of symptoms
- Pain is the major symptom associated with SSS
- The pain is predominantly centres over the superior-medial (upper edge of the shoulder blade)
- Some people can feel the pain deep to the shoulder blade
- There is often associated pain radiating up into the trapezius and rhomboid muscles and can affect the neck
- The pain is often worse on movements of the shoulder blade and can be worse at night
- Snapping / Crepitus is usually also present
- The severity of the crepitus can vary and is not necessarily proportional to the amount of pain that someone is experiencing.
- In certain circumstances it can be very loud and cause significant issues with movement and in others it can be much less severe
- Shoulder Girdle functional disturbance
- In certain situations, a combination of the snapping of the scapula and the associated pain can affect the function of the muscles surrounding the scapula. This, in turn, can affect the way in which the muscles are able to function and can lead to a Scapula Dyskinesia
- If the scapula is not moving or functioning correctly this can have a secondary effect on the Glenohumeral joint. This can lead to problems with secondary rotator cuff tendonitis and instability
- Onset of Symptoms


- How do you Diagnose Snapping Scapula Syndrome?
- Snapping Scapula
- A diagnosis of SSS is mainly based on the clinical symptoms and findings
- Whilst many people have a Snapping Scapula (crepitus) although they have the crunching and there is an audible sound, they do not have any problems with pain or function. They do not have a clinical problem and do not have symptoms
- SSS is diagnosed in patients who have a Snapping Scapula but also have problems with pain over the superior medial pole of their scapula with associated problems with shoulder function
- Diagnostic / Therapeutic Ultrasound Guided Cortisone Injection
- An Ultrasound Scan can be undertaken by a radiologist to look at the area between the undersurface of the scapula and the chest wall
- The advantage of an USS is that it is dynamic and it is possible to visualise what happens as the scapula moves over the chest wall
- In patients that have SSS there is often scar tissue or inflamed bursal tissue between the scapula and the chest wall
- If this is present it is possible to undertake a guided injection of local anaesthetic and cortisone into this area
- If the source of the pain is coming from this point patients may notice an immediate benefit from the local anaesthetic. This is diagnostic of a SSS
- MRI Scan
- An MRI scan of the posterior chest wall can visualise the scapula, the muscles that are attached to it and the chest wall below
- Although there are some features on an MRI scan that might ‘suggest’ SSS they are not diagnostic
- CT Scan
- A CT scan is able to show the 3D anatomy of the scapula
- Although previously it was thought that there are some features on a CT scan that are specific to SSS this is not actually the case
- However, a CT scan is able to assess any other unusual anatomical variants or associated pathology (osteochondroma)
- Snapping Scapula

Treatment for Snapping Scapula Syndrome
- Analgesia/Pain Relief
- pain is the most prominent problem associated with SSS before it is possible to undertake any proper rehabilitation the pain needs to be under control
- NSAID (Non-Steroidal Anti-Inflammatories)
- NSAIDs work be reducing the pain associated with inflammation around the scapula
- NSAIDs can damage the stomach lining and affect the kidneys. It is important that a patient’s Family Doctor prescribes this medication if it is going to be used for a longer term
- Codeine based Analgesics
- Codeine based analgesics are pain killers and affect a patient’s perception of pain. As a result, they can have some effect on consciousness depending on their strength
- Codeine based analgesics can lead to constipation if taken for a longer time. Having a high-fibre diet or even taking laxatives might need to be considered
- Nociceptive Analgesics
- Nociceptive pain killers work on nerve generated pain
- In certain types of SSS there can be a neurogenic component to the pain
- Amitriptyline in lower doses works as a nociceptive pain killer. It has a useful side-effect in that it can make patients drowsy
- in cases of severe pain Amitriptyline can be prescribed at night
- Physiotherapy
- The initial treatment for SSS is structured scapula stabilising programme
- This type of physiotherapy usually has to be undertaken by a Physiotherapist that specialises in shoulder conditions
- Even when physiotherapy works it can take can often take many months of sustained exercises
Find out more about Shoulder Physiotherapy…. (Patient Information – Physiotherapy – Physiotherapy
-
-
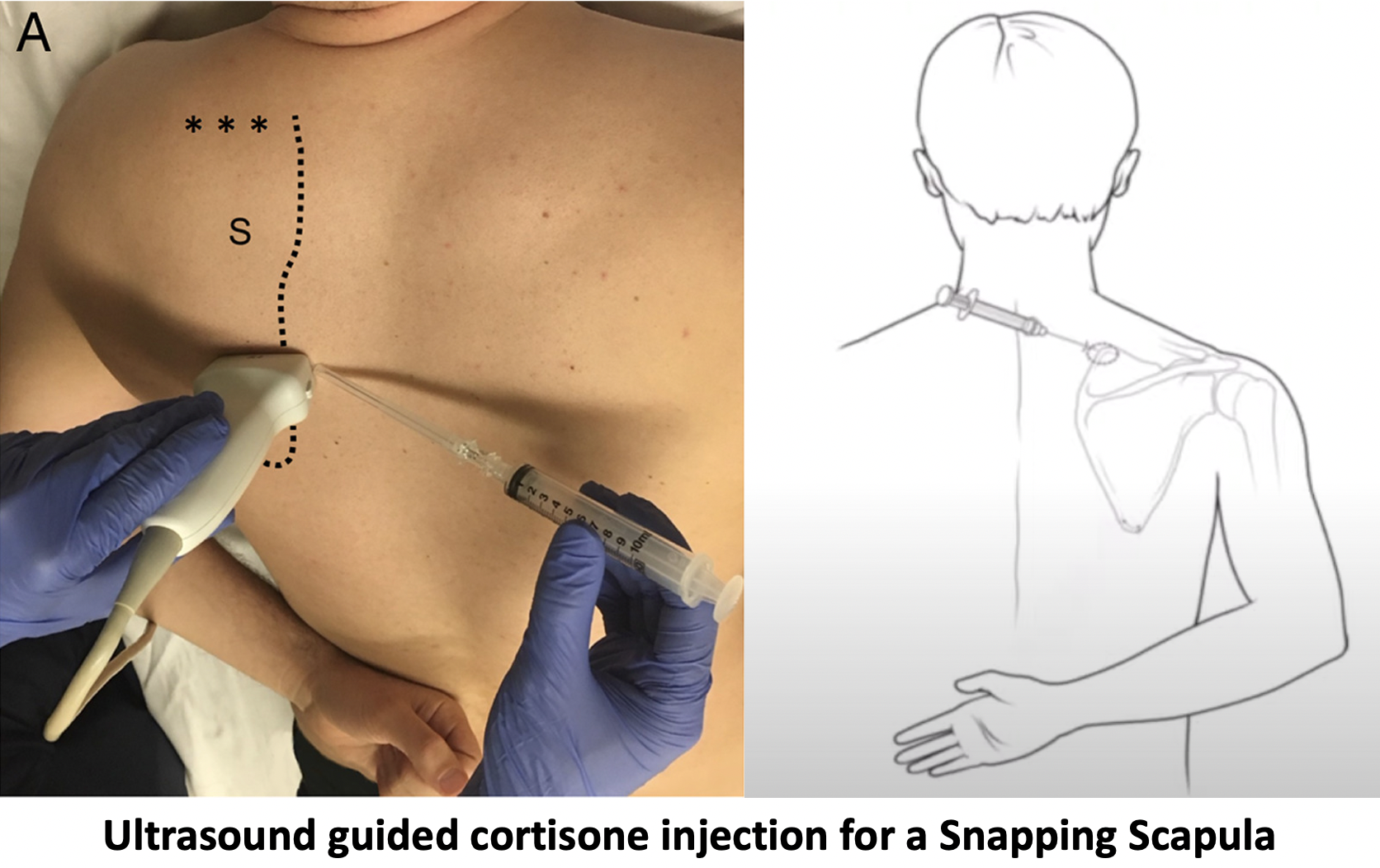
- Ultrasound Guided Subs-Scapular Cortisone Injection
- If despite optimal oral analgesics and an adequate course of physiotherapy pain continues to be a problem a Cortisone injection may be considered
- Cortisone is a corticosteroid that is natural produced by the body’s Adrenal Gland. Injectable cortisone is synthetically produced and has a very powerful anti-inflammatory action. When injected into the Sub-Scapular space it has the potential of settling severe inflammation, allowing patients to undertake their rehabilitation exercises
- To place the injection exactly into the correct position, due to the relative inaccessibility of the subscapular space, I prefer to ask the radiologists to undertake the injection by ultrasound guidance
- As the pain symptoms in SSS can be caused by either inflammation or a neurogenic cause, or a combination of both, a Cortisone injection will only relieve the inflammatory component
- As the components of pain can vary between patients with SSS the beneficial effect of a Cortisone injection can vary from a complete resolution of pain to a minimal benefit
- Ultrasound Guided Subs-Scapular Cortisone Injection
-


Surgery for Snapping Scapula Syndrome
- Whilst the majority of patients with SSS can be successfully treated with the treatments described above, there are some patients that continue to experience significant problems despite optimal non-operative treatment
- In this situation the further options available are to either continue with the symptoms as they are or the consider surgery
- The surgery is aimed a relieving the pain associated with SSS, it is not specifically aimed at removing
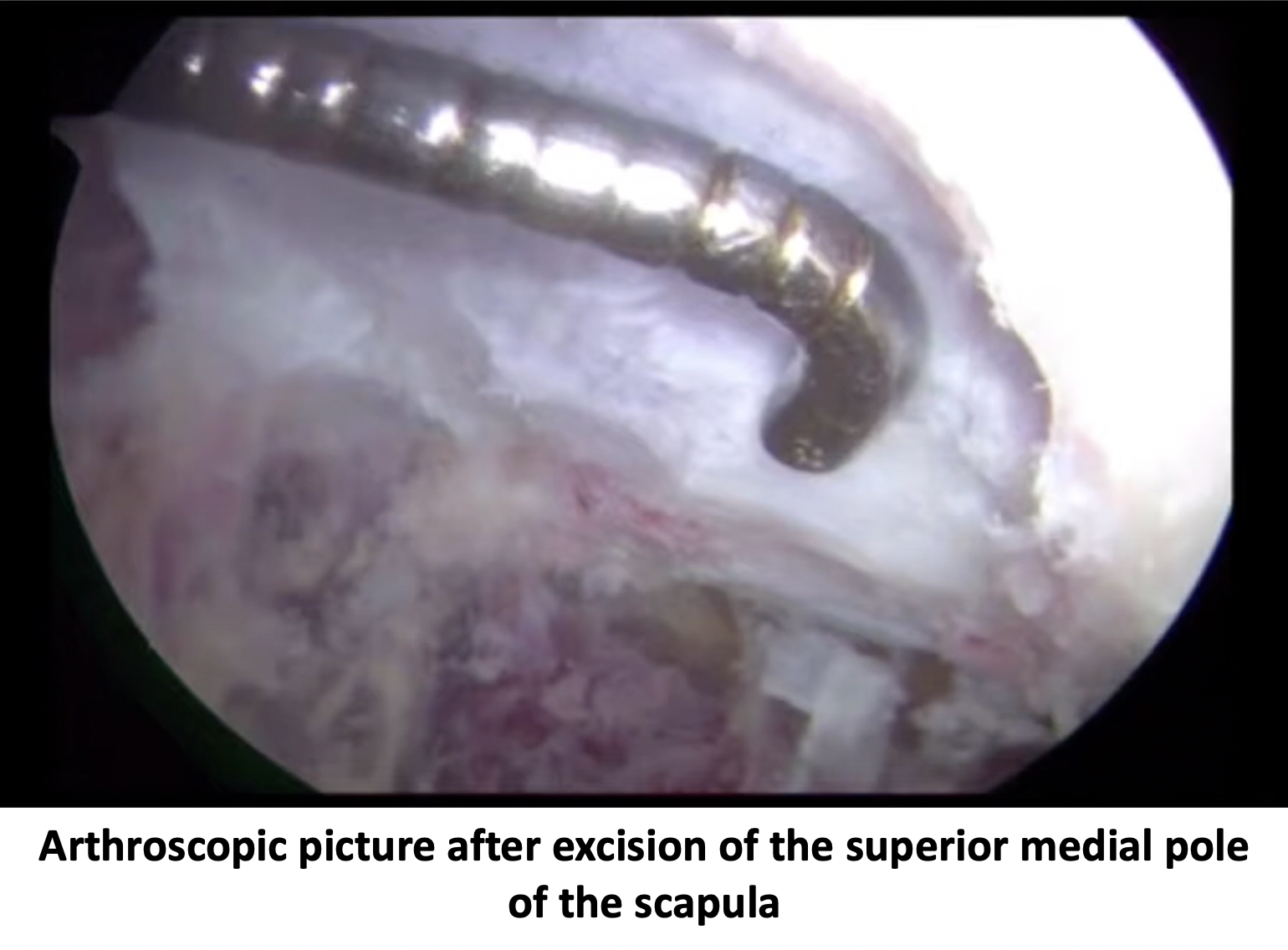
Arthroscopic Scapulothoracic Surgery
An Arthroscopic Scapulothoracic surgery is undertaken with a general anaesthetic as an In-Patient procedure either as a day case or as a one-night stay. The surgery aims to remove any inflamed or scarred tissue lying between the superior medial pole of the scapula and the chest wall. At the same time about 2 cm of the bone at the superior medial pole of the scapula is excised to increase the clearance space and prevent a further recurrence of the symptoms.
The video below describes the surgical technique.
Watch a video of an Arthroscopic Capsular Release…. (Research & Education – Video – Frozen Shoulder)
Find out more about Arthroscopic Shoulder Surgery… (Patient Information – Arthroscopic Shoulder Surgery)
Find out more about having an anaesthetic…. (Patient Information – Having an Anaesthetic – General Anaesthetic)
The video below describes the surgical technique.


After the Surgery
Post-Operative Care
Following an Scapulothoracic Arthroscopy the patient, depending on the time of day when the procedure is undertaken and who the patients recovers from the anaesthetic, can be done as either a Day Case procedure or as an overnight stay in hospital. I would see the patient after the surgery to discuss how the procedure has gone and arrange for further follow-up. The patient will be seen by the In-Patient Physiotherapy team and undergo several sessions of intensive physiotherapy before going home. Further Out-Patient physiotherapy will then be organised.
Find out more about Physiotherapy following Shoulder Surgery…. (Patient Information – Physiotherapy – Physiotherapy-Frozen Shoulder)
I would usually review patients in the clinic 1 month and 3 months after their procedure to assess their progress and recovery.
Rehabilitation Protocol
Immediately after the surgery, when the patient has woken up from their general anaesthetic, their scapula and shoulder and arm will be numb from local anaesthetic administered at the time of surgery. Patients can begin to move their scapula, shoulder and arm immediately although they are given a sling to wear incase their scapula becomes uncomfortable. I encourage patients to try and use their shoulders as much as possible to try and regain movement.
My standard rehabilitation protocol is outlined below. The information and time to recovery are a general estimation and may vary from person to person. My advice to most patients is to try and organise to be off of work for 1 – 2 weeks after the surgery. This is so that they can be as diligent as possible in doing their exercises. The physiotherapsits would usually recommend that patients initially do exercises every hour that they are awake.
| Post op | |
| Immediate |
|
| Day 1-3
Weeks |
|
| 3-6 Weeks |
|
| Milestones | |
| Week 3 | Full passive range of movement |
| Week 6 | Full active range of movement, good scapular control |
Return to Functional Activities
Driving Once ROM and muscular power
restored & patient feels safe
Swimming As pain allows
Golf 6 weeks
Racquet Sports/Repeated 2-3 months
Overhead Activities
Lifting As able
Work Sedentary - As able
Manual - 6 weeks, may need to modify activity for 3 months
Success of Surgery, Risks & Complications
A Scapulothoracic Arthroscopy for SSS is usually a very successful procedure for settling the pain component but, because the surgery only frees up the space beneath the superior medial pole of the scapula and relieves the pain, it usually takes between 3 – 6 months for the muscles, ligaments and tendons to fully recover and for the Scapula tracking to return to normal. Often patients do not notice a significant improvement in the actual snapping sensation, but their pain disappears and their function returns. For a standard Scapulothoracic Arthroscopy >90% of patients’ will be happy with their shoulders after 6 months.
There are always risks and complications associated with any operation.
- Anaesthetic - The risks of having a General Anaesthetic and an Interscalaene Nerve Block are very low, but will always need to be assessed on an individual basis by an Anaesthetist. Suffice it to say, that whilst a Shoulder Operation can in no way be considered a ‘life-saving’ procedure, an Anaesthetist would not consider undertaking an anaesthetic if they had any concerns that an undue risk was being taken.
- Infection – Infection following arthroscopic surgery is rare < 0.2%
- Neurovascular Injury – Damage to significant neurovascular structures during arthroscopic shoulder surgery is rare < 0.2%
- CRPS Type 1 – A Chronic Pain Syndrome following arthroscopic shoulder surgery is rare < 0.2%
Scapula Dyskinesia
-
- Scapula Dyskinesia
- a disturbance with the co-ordinate sequence of the stabilising muscles as they move the Scapula
- the glenoid (shoulder socket) is part of the scapula. If the scapula is not moving correctly or is not stable, this can have a significant effect on glenohumeral joint function
- Types of Scapula Dyskinesia
- There are 4 types of Scapular Dyskinesia
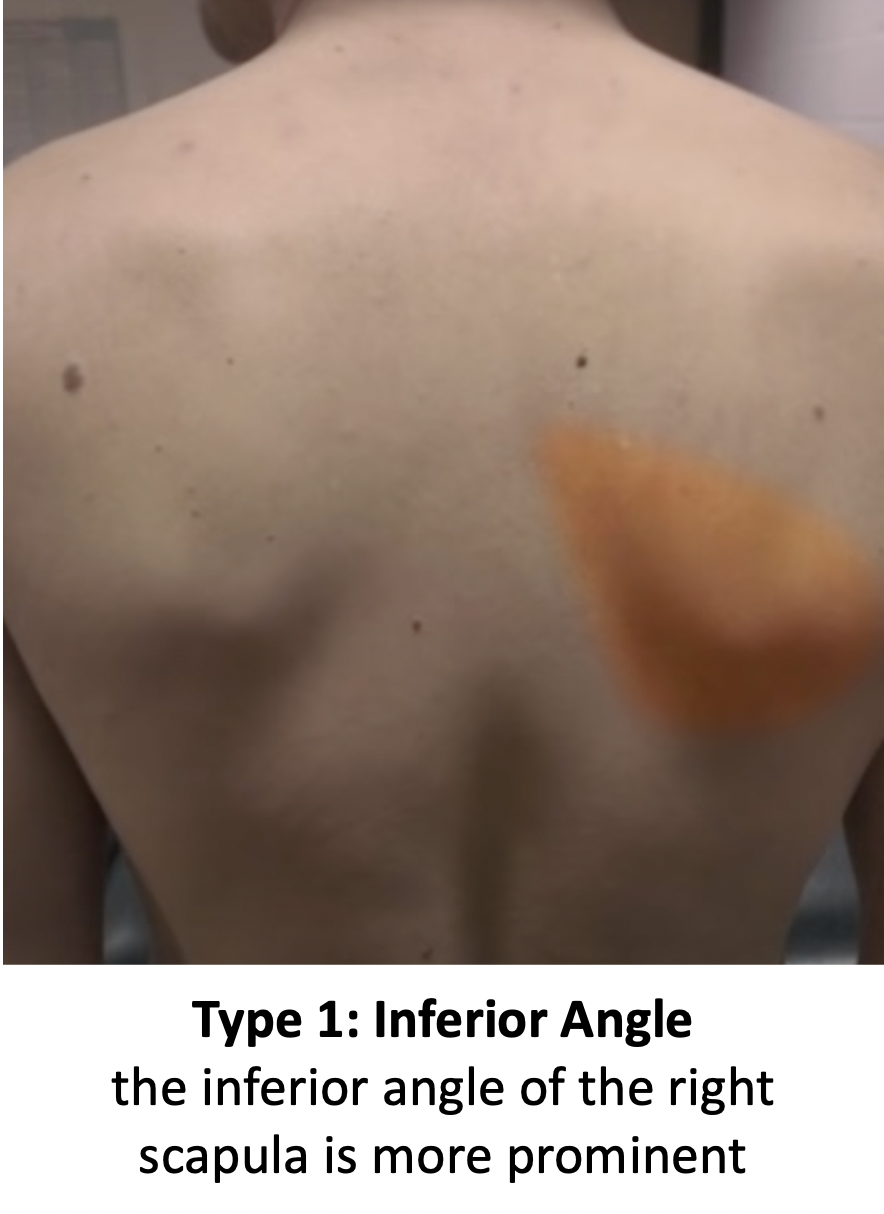
- Type 1 – Inferior Angle
- at rest the inferior medial border is prominent backwards
- during motion the inferior angle tilts backwards and the acromion tilts forwards over the thorax
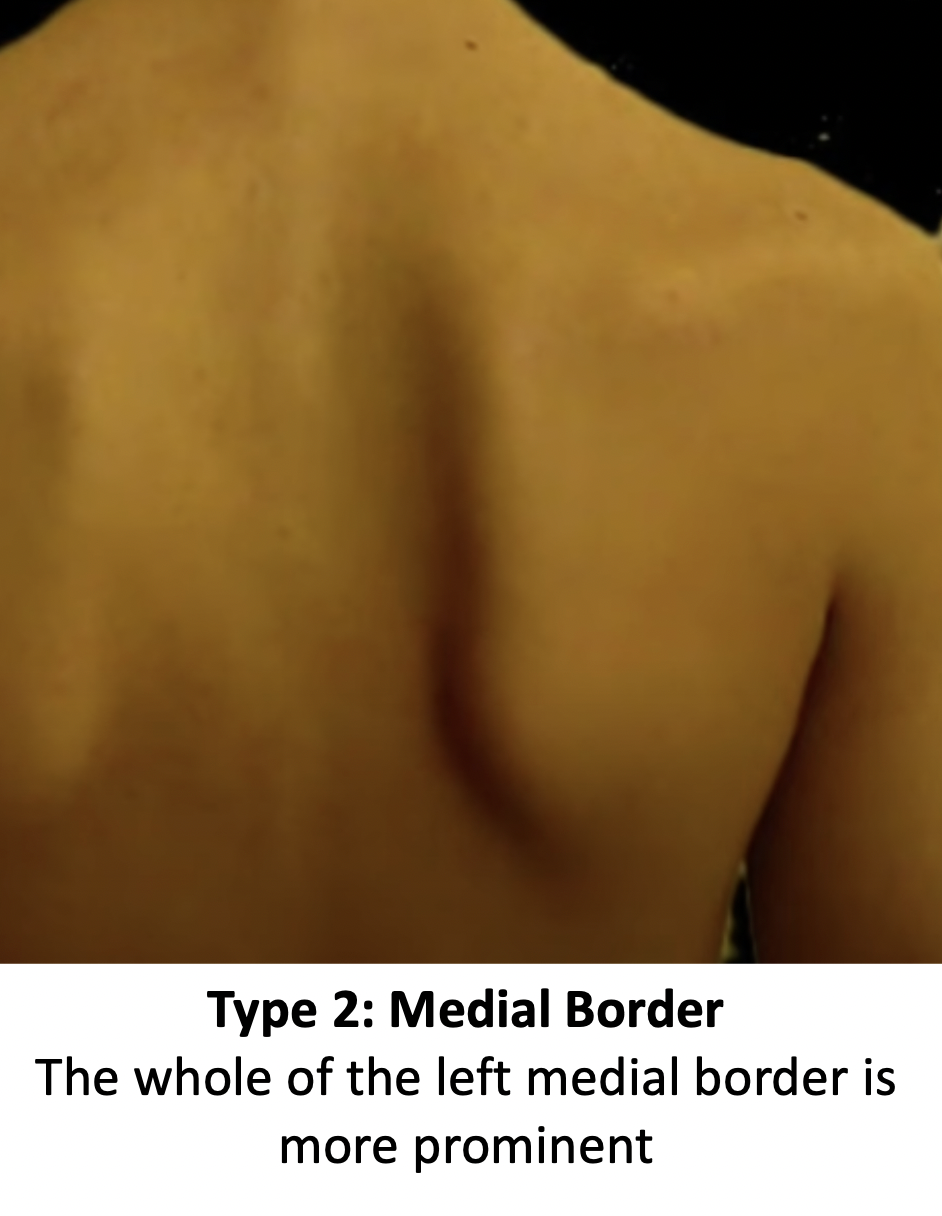
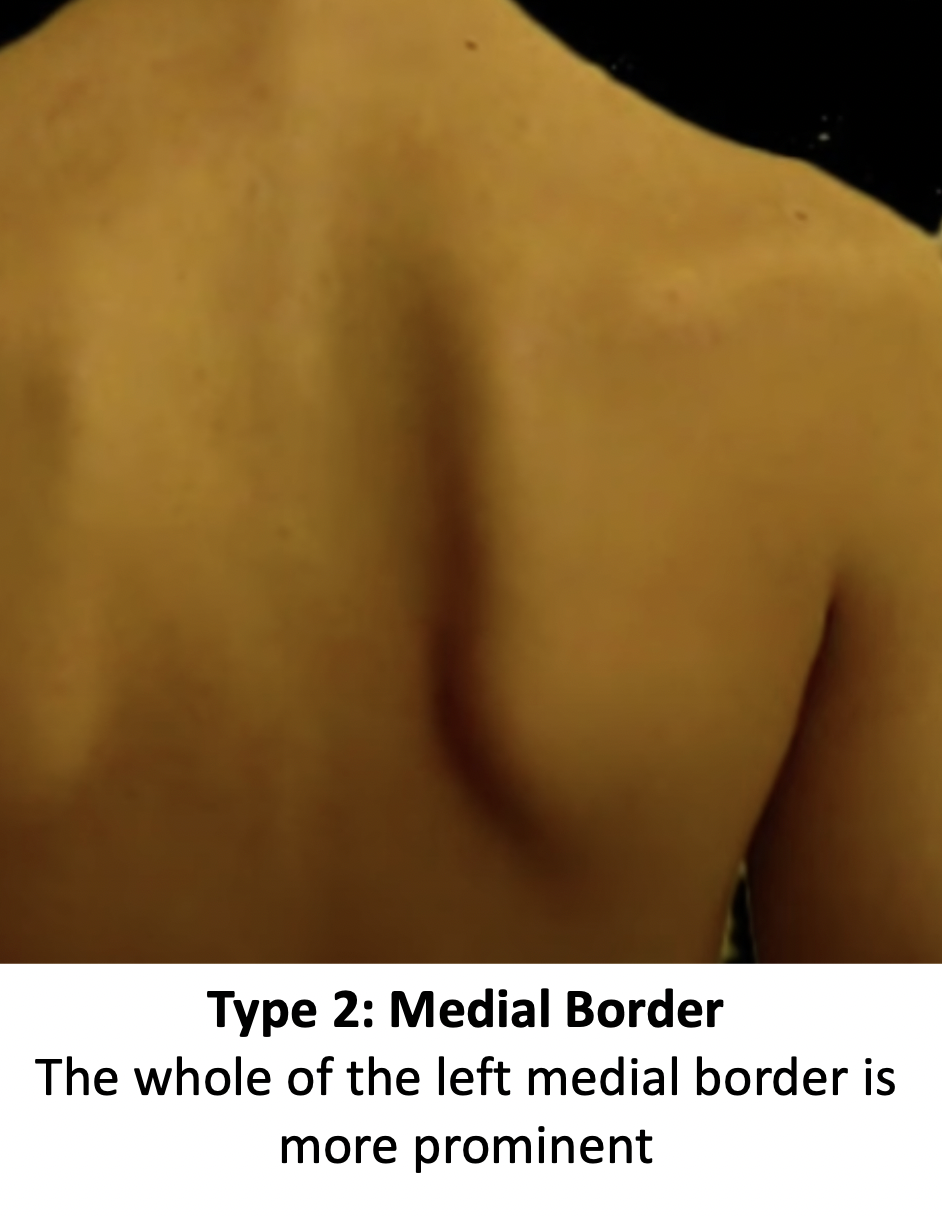
- Type 2 – Medial Border
- at rest the entire medial border is prominent backwards
- during motion the medial border tilts backwards off of the chest wall
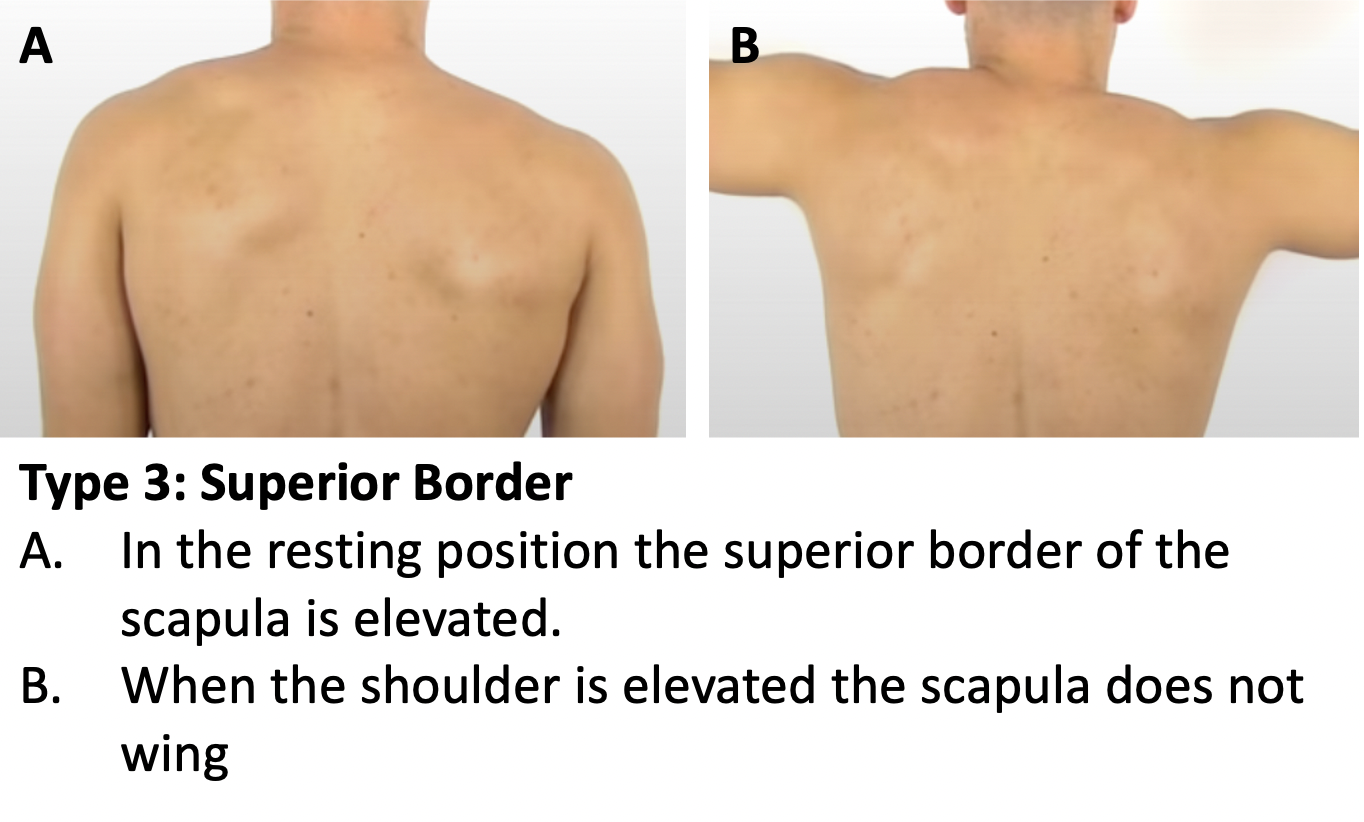
- Type 3 – Superior Border
- at rest the superior border is superiorly elevated and the entire scapula is displaced anteriorly
- during motion a shoulder ‘shrug’ is required to initiate movement without winging of the scapula
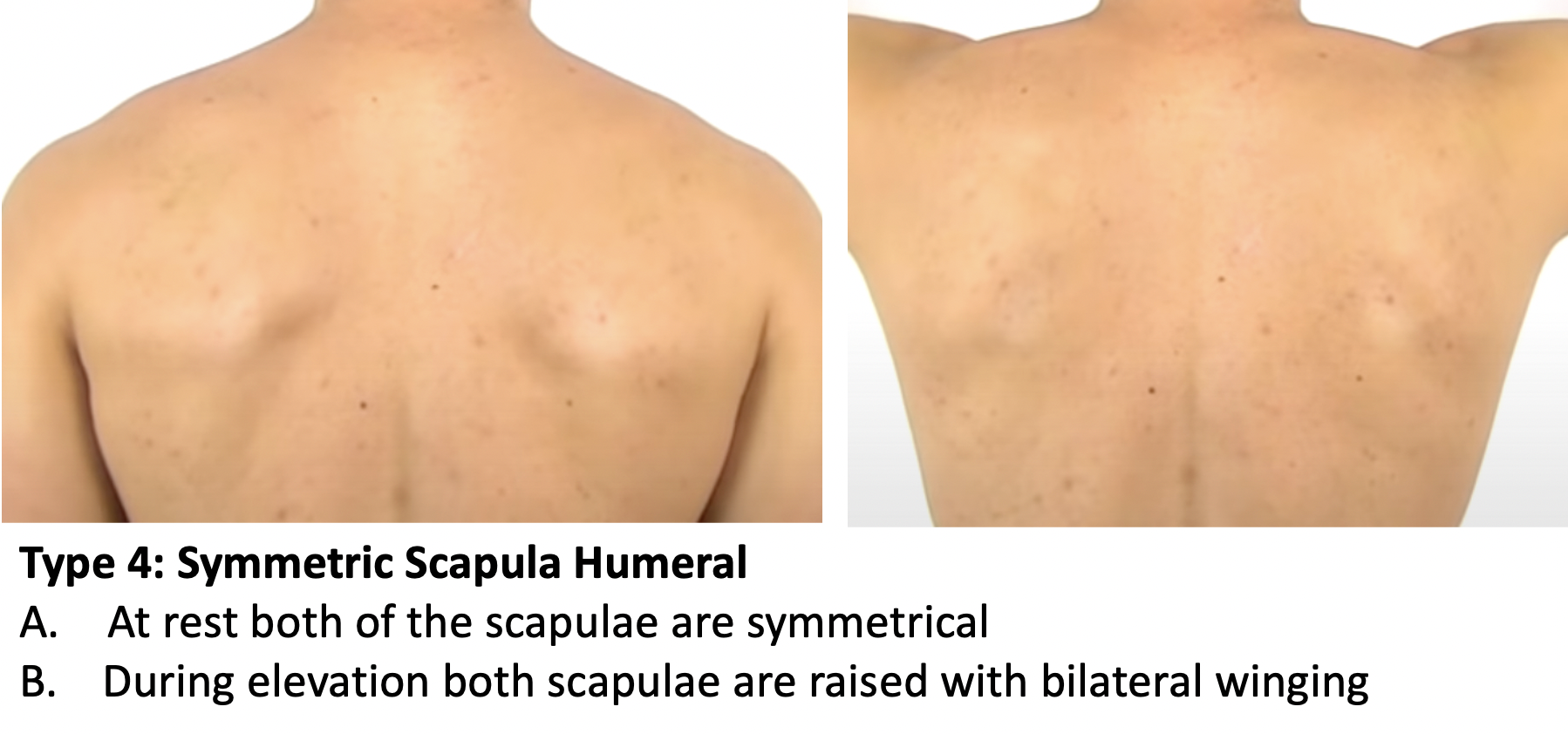
- Type 4 – Symmetric Scapula Humeral
- at rest both scapulae are symmetrical
- during motion there is symmetrical upward rotation with bilateral winging
- Diagnosis
- The initial diagnosis of Scapula Dyskinesia is purely clinical and made by observation
- Scapula Dyskinesia is due to a muscle imbalance between the scapular stabilising, this is most commonly due to a weakness/imbalance of one group of stabilising muscles, this maybe due to,
- weakness in core muscles
- secondary to compensation for a glenohumeral joint problem
- damage to the muscles
- abnormality of the shape of the scapula (secondary to trauma)
- nerve damage
- The majority of Scapula Dyskinesia cases are due to weakness of the core muscles and/or an associated glenohumeral joint problem (instability, rotator cuff or osteoarthritis)
- Depending on the clinical examination and assessment of the glenohumeral joint further investigations may be required (MRI, CT, nerve conduction studies
- Scapula Dyskinesia
-
- Treatment
- Successful treatment of Scapula Dyskinesia involves treating the specific muscle group imbalance around the scapula and also addressing any other precipitating cause (shoulder instability or rotator cuff problems) at the same time
- Treating the specific Scapula stabilising muscle imbalance requires highly specialist physiotherapy input, which is beyond the remit of this site
- Treatment
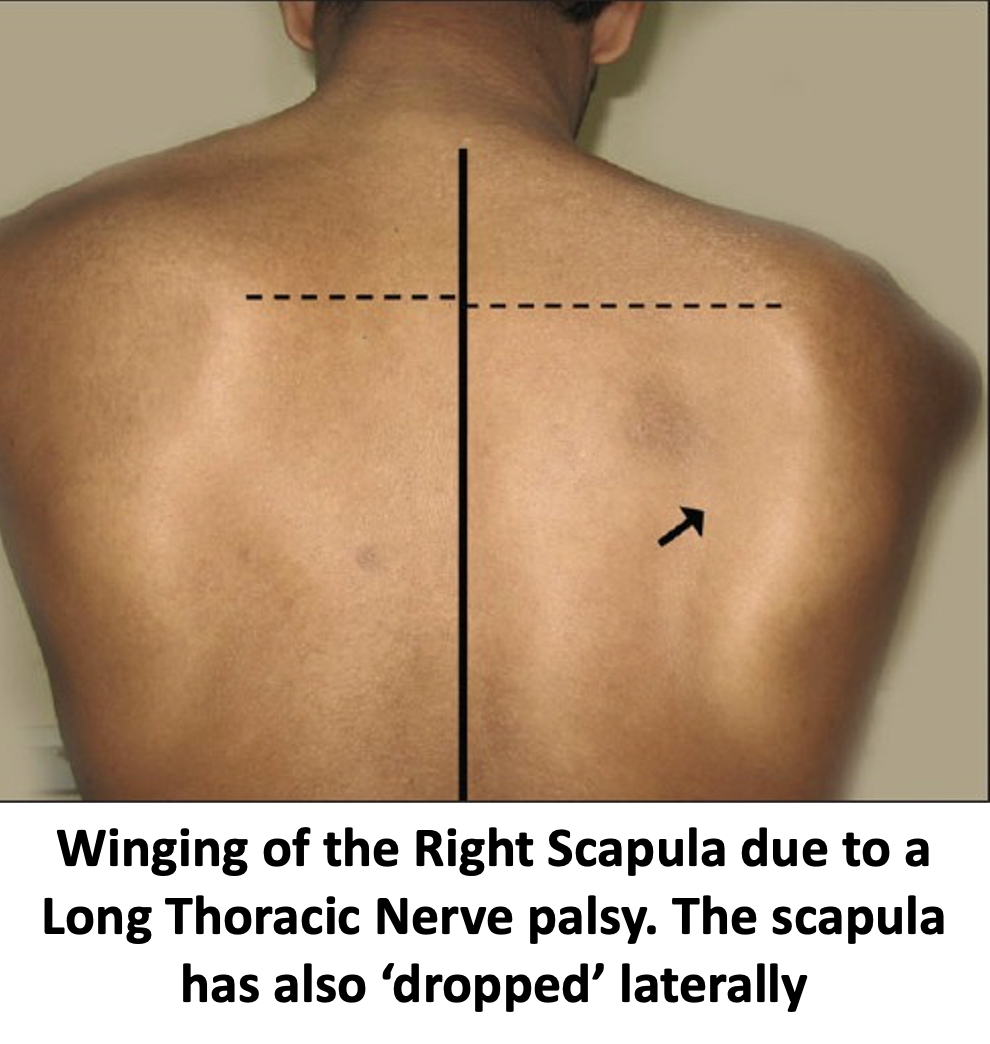
Nerve Injuries & Winged Scapula
- nerve injuries and problems around the shoulder girdle are rare but can occur
- the commonest nerve to be affected are the Long Thoracic Nerve and the Spinal Accessory Nerve
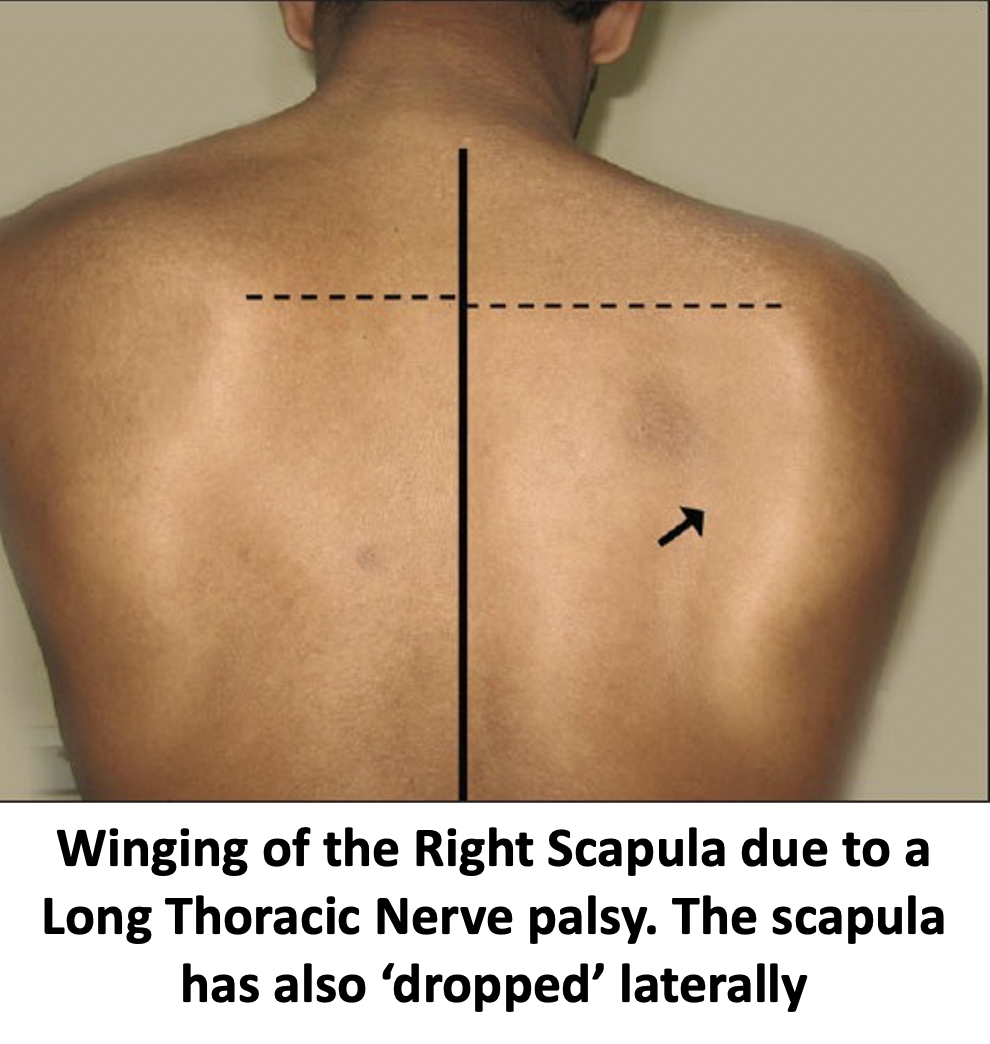
- damage to either of these nerves can affect shoulder function, particularly with the scapula resulting in Scapula Winging
Long Thoracic Nerve
- the long thoracic nerve supplies the motor function to the serratus anterior muscle
- paralysis of serratus anterior leads to winging of the scapula (Type 2 Scapula Dyskinesia)
- There are a number of causes for a Long Thoracic Nerve injury/palsy
- Traumatic
- Traction Neuropraxia – this is the most common cause and is due to the result of the long thoracic nerve being stretched. This can occur following a single ‘one off’ injury or can be the result of a sustained load (such as wearing a heavy rucksack for a sustained length of time or using under arm crutches)
- Damage to the thoracic nerve due to a fracture around the clavicle or scapula
- Iatrogenic injury during surgery around the neck and chest
- Non-Traumatic
- Viral illness
- Muscular Dystrophy
- Parsonage-Turner Syndrome
- Traumatic
- Diagnosis
- The initial diagnosis is made by taking a History, to assess whether there might have been a precipitating cause or event, and clinical examination
- EMG Studies – electromygraphic studies are undertaken by a Nureophysiologist and are able to assess the function of specific nerves
- EMG studies can detect whether there is a Neoropraxia (temporary damage to a stretched nerve), it’s probable cause and its likelihood of recovering or whether there is a more serious injury
- Treatment
- The vast majority of Long Thoracic Nerve are due to a neuropraxia and are likely to recovery
- Neuropraxia - nerve recovery following a neuropraxia is very slow. The nerve has to ‘re-grow’ from the point of injury and does so at 1mm per day
- The average nerve is 15 – 20 cm long so recovery can take up to 1 year
- During the recovery period Physiotherapy is very important to help the non-affected surrounding muscles and the recovering Serratus Anterior
- Nerve Damage / Transection – if the nerve has actually been damaged then surgery to attempt to repair the nerve is the best course of action.
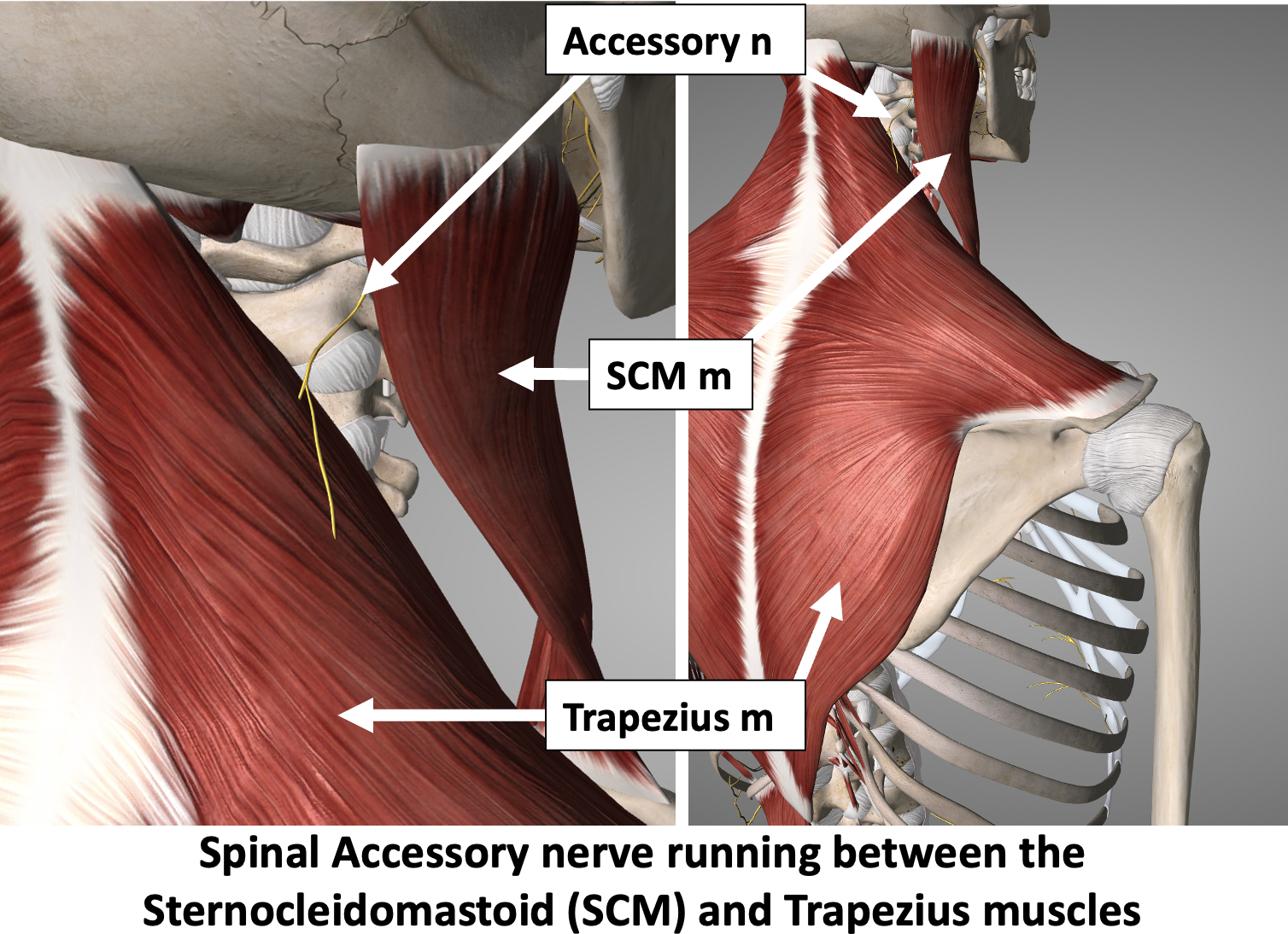
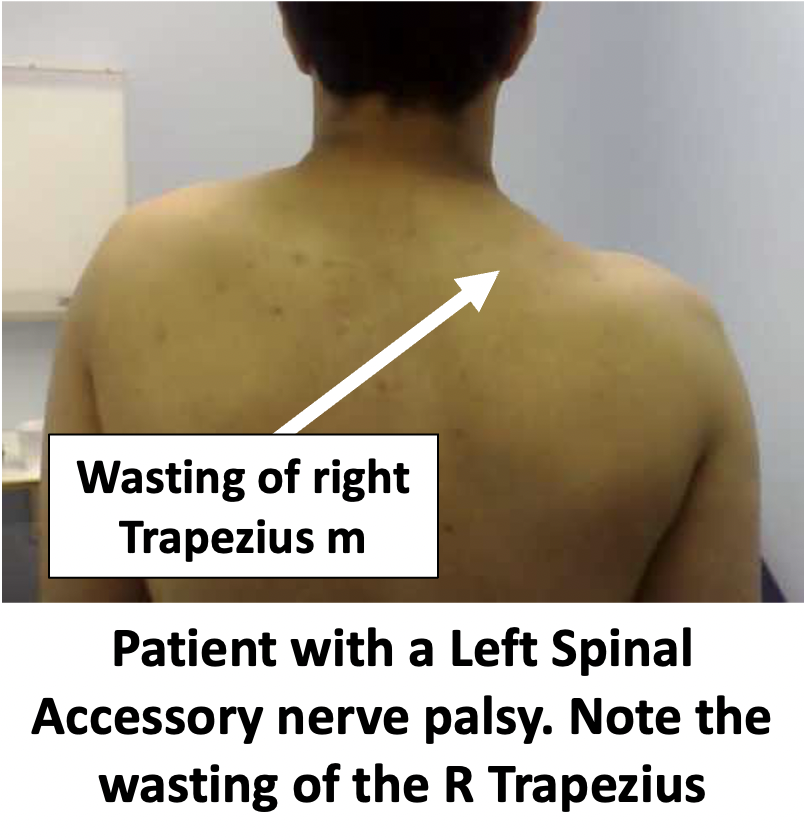
Spinal Accessory Nerve
- The Spinal Accessory Nerve supplies the motor function to the Sternocleidomastoid and Trapezius muscles
- Injury to the spinal accessory nerve can lead to drooping of the shoulder and winging of the scapula
- There are a number of causes of a Spinal Accessory nerve injury/palsy
- Traumatic
- the most common cause is damage to the nerve during surgery (neck dissection & cervical lymph node dissection)
- Non-Traumatic
- Viral illness
- Traumatic
- Diagnosis
- The initial diagnosis is made by taking a History, to assess whether there might have been a precipitating cause or event, and clinical examination
- EMG Studies – electromygraphic studies are undertaken by a Nureophysiologist and are able to assess the function of specific nerves
- EMG studies can detect whether there is a Neoropraxia (temporary damage to a stretched nerve), it’s probable cause and its likelihood of recovering or whether there is a more serious injury
- Treatment
- The vast majority of Spinal Accessory Nerve injuries result in a fairly modest winging of the scapula which often does results in only a minor functional deficit and often does not warrant treatment
- For patients with a significant Trapezius functional deficit (which is very rare) there are muscle transfer operative procedures that can improve function