Arthroscope & Visualisation
To visualize the inside of the shoulder requires a long lense & probe, a powerful light source, a video camera and a TV monitor.
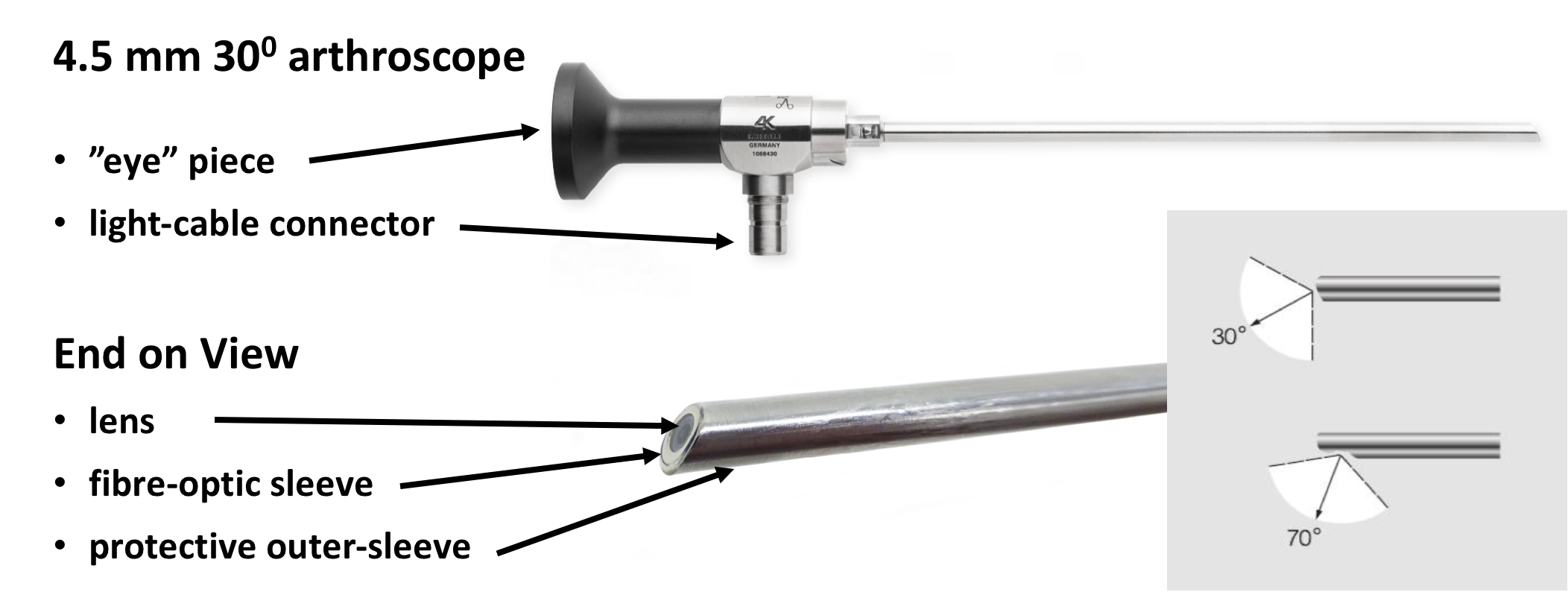
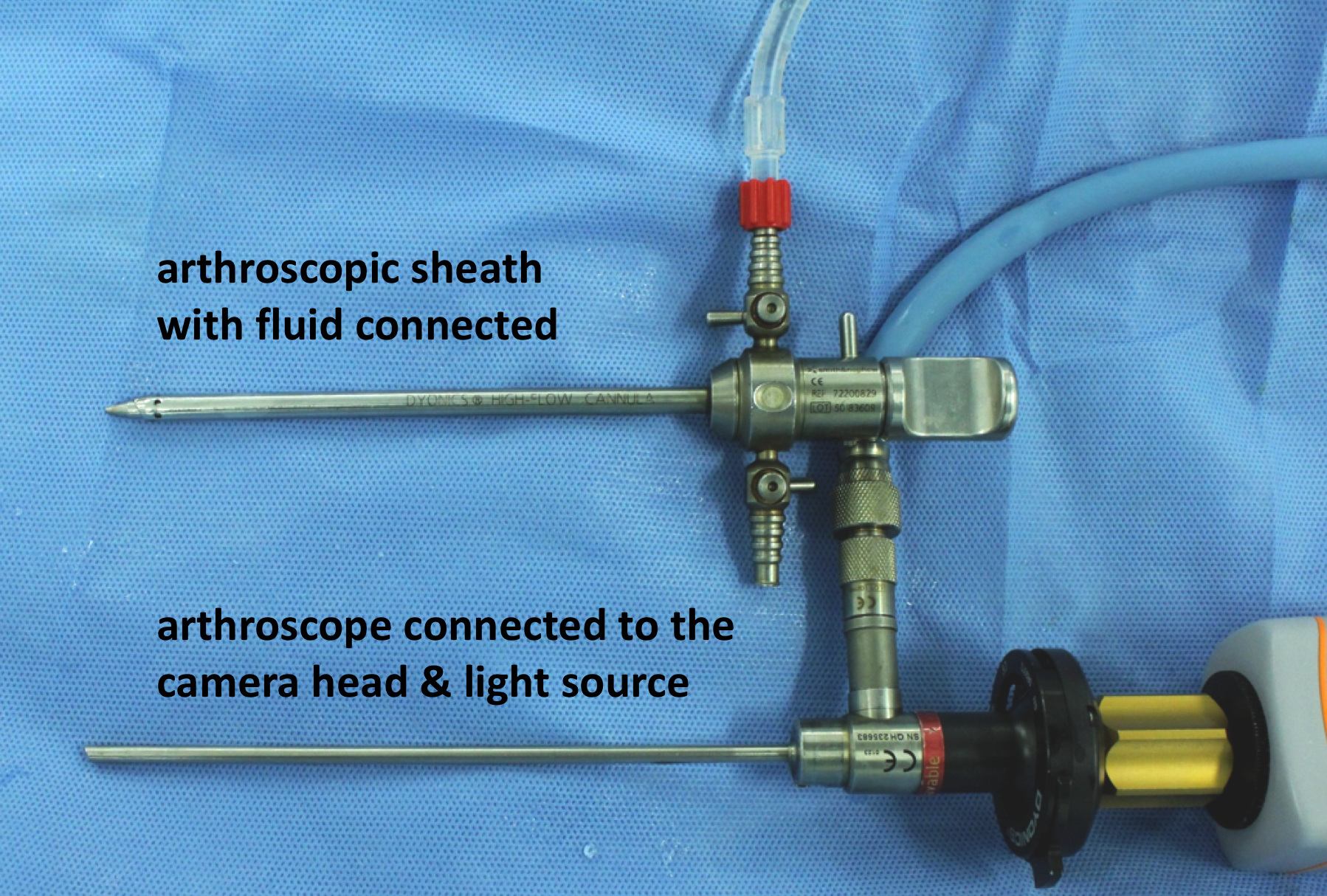
- The Arthroscope – the arthroscope is essentially a slim telescope (about 25cm in length) around which it is surrounded by a thin fibre-optic tube. Standard arthroscopes are 4.5mm or 2.9mm in diameter. At one end is the ‘eye-piece’ or video connection and at the ‘patient’ end there is a lens. The lens can be angled at either 300 or 700 to allow a larger field of view as the scope is rotated. A powerful light- cable is attached to the side of the arthroscope to illuminate the joint via the fibre-optics. The arthroscope is usually inserted into the joint through protective sheath that allows for the arthroscope to be taken in and out of the joint
- The Camera & Monitor- the end of the arthroscope is connected to a high resolution HD camera. This is connected by a cable to an HD monitor and computer. The arthroscopic image is then viewed off of the monitor. The camera has focusing and zoom controls and the computer is able to record and store both still and video images of a procedure
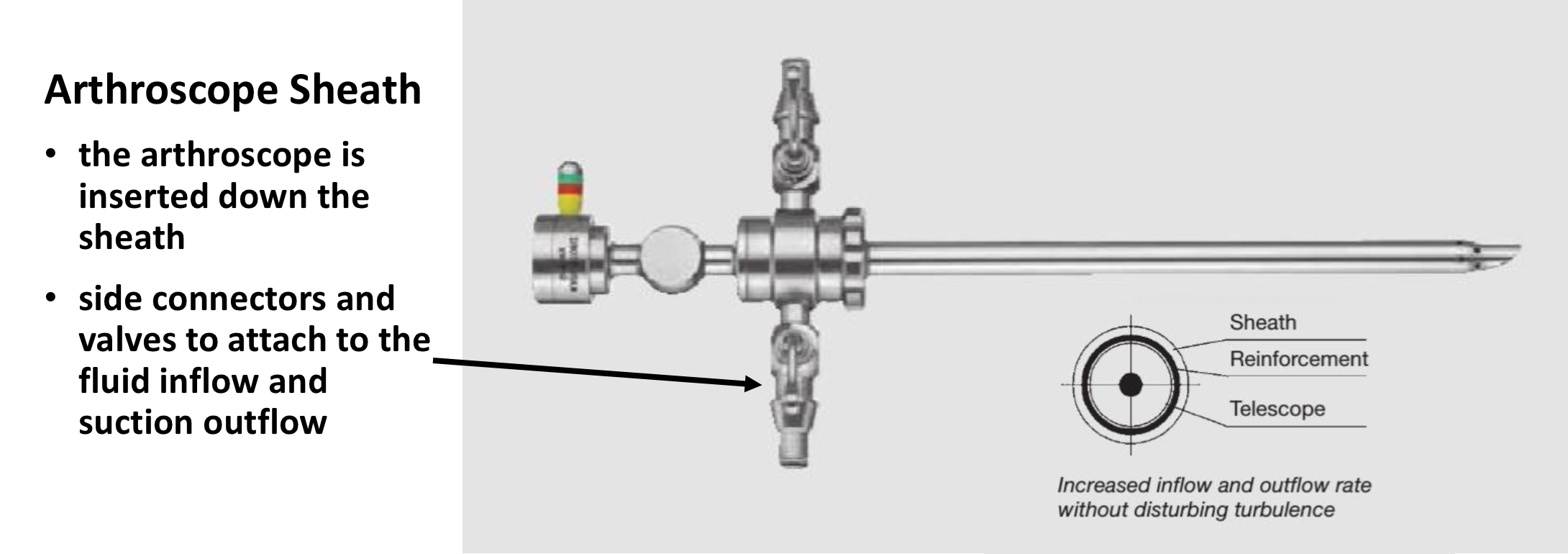
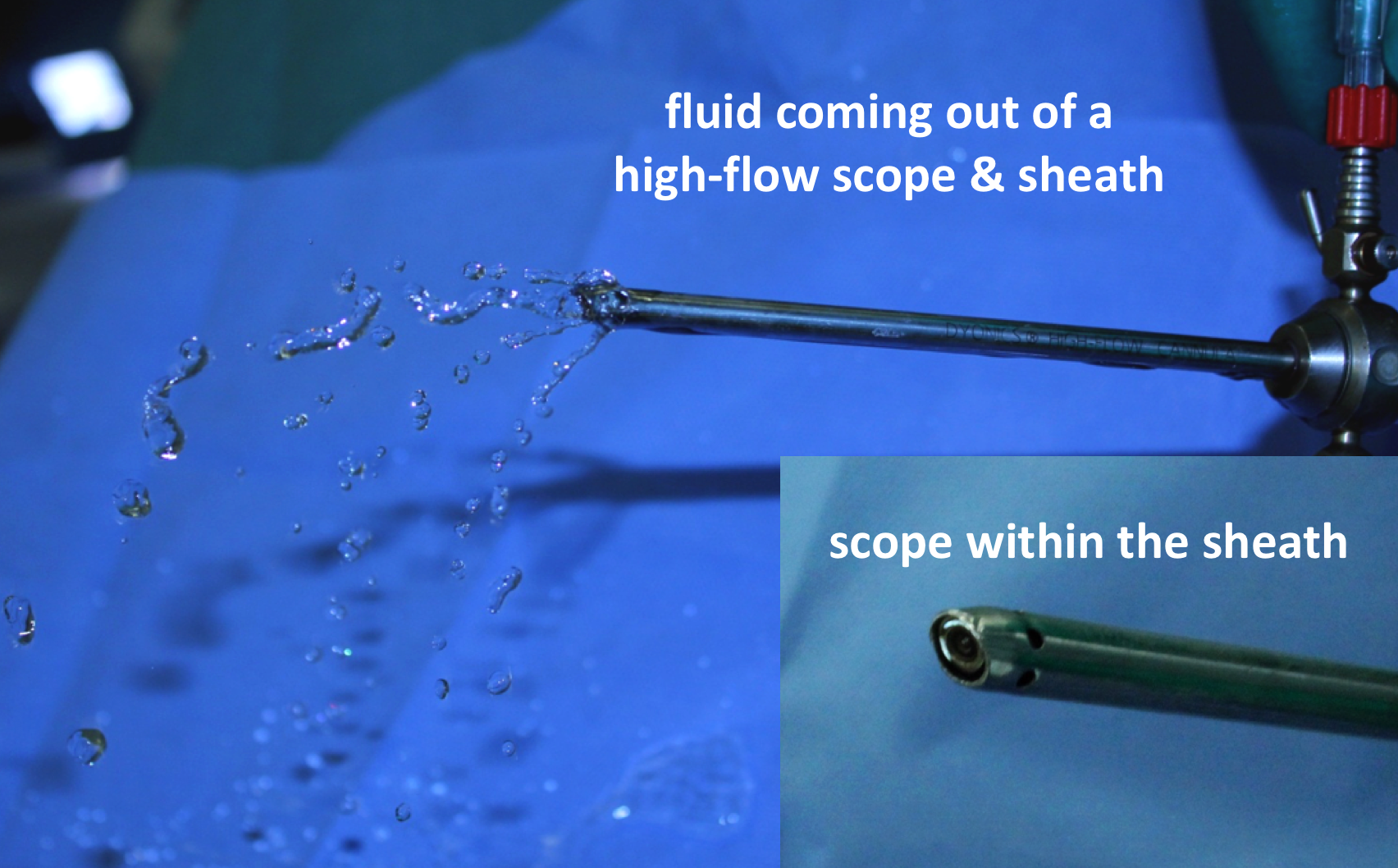
- The Arthroscope Sheath & Fluid Control - In order to see inside a joint and to undertake any procedures the joint needs to be ‘opened’ up. This is done by distending the joint with normal saline fluid. The fluid is introduced into the joint through the sheath. This is essentially a metal tube that is 6.5mm in diameter down which the 4.5mm arthroscope is inserted. Through a valve, at the top of the Obturator sleeve, fluid can be introduced down the side of the arthroscope into the joint
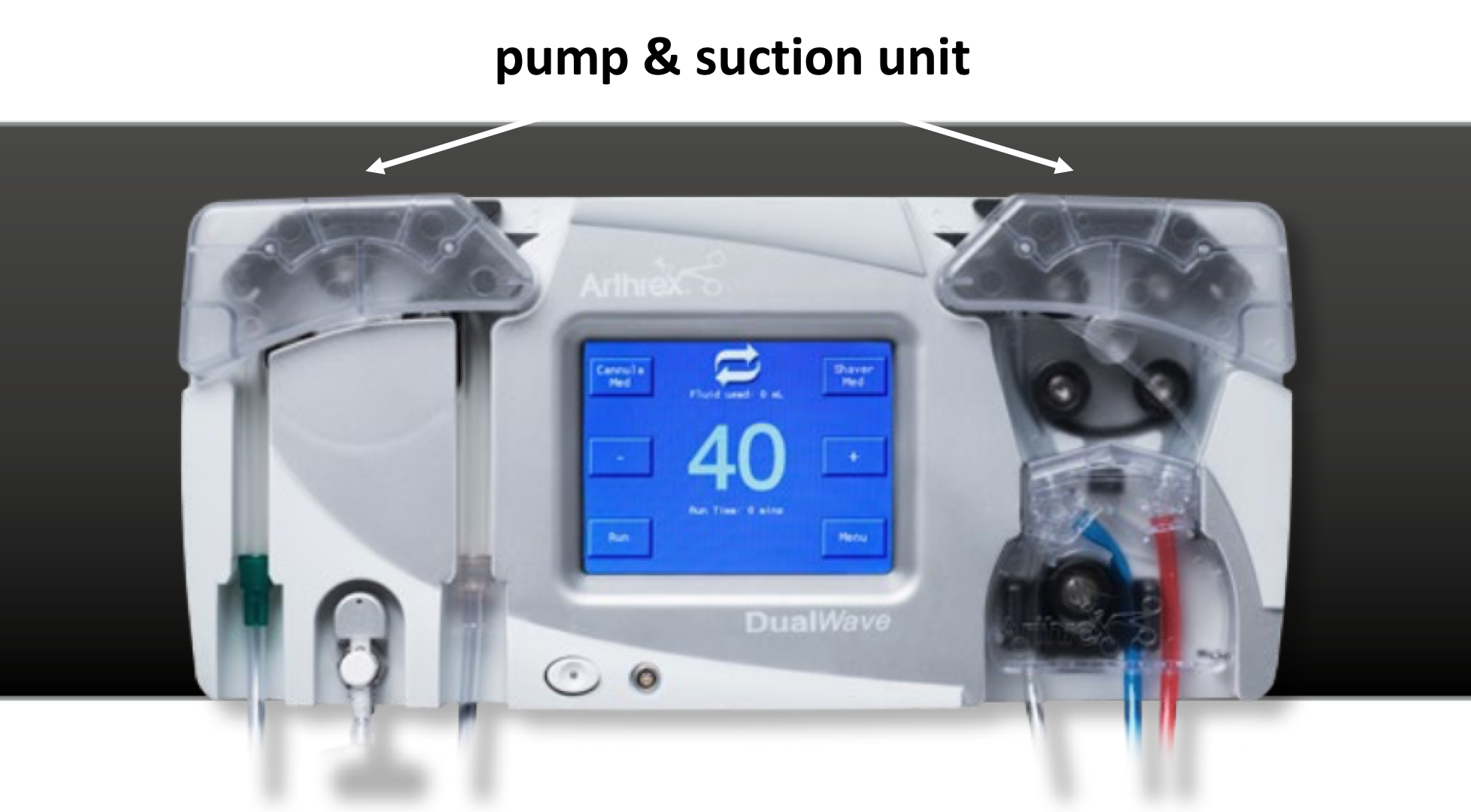
- The Pump & Fluid Control - A specialized pump is used to control the pressure and rate of fluid going into the joint. It usually also has a suction control system that is linked to any of the power-instruments that are used. It is then able to adjust the rate of input and output of fluid into the joint and maintain a constant pressure to optimize visualization
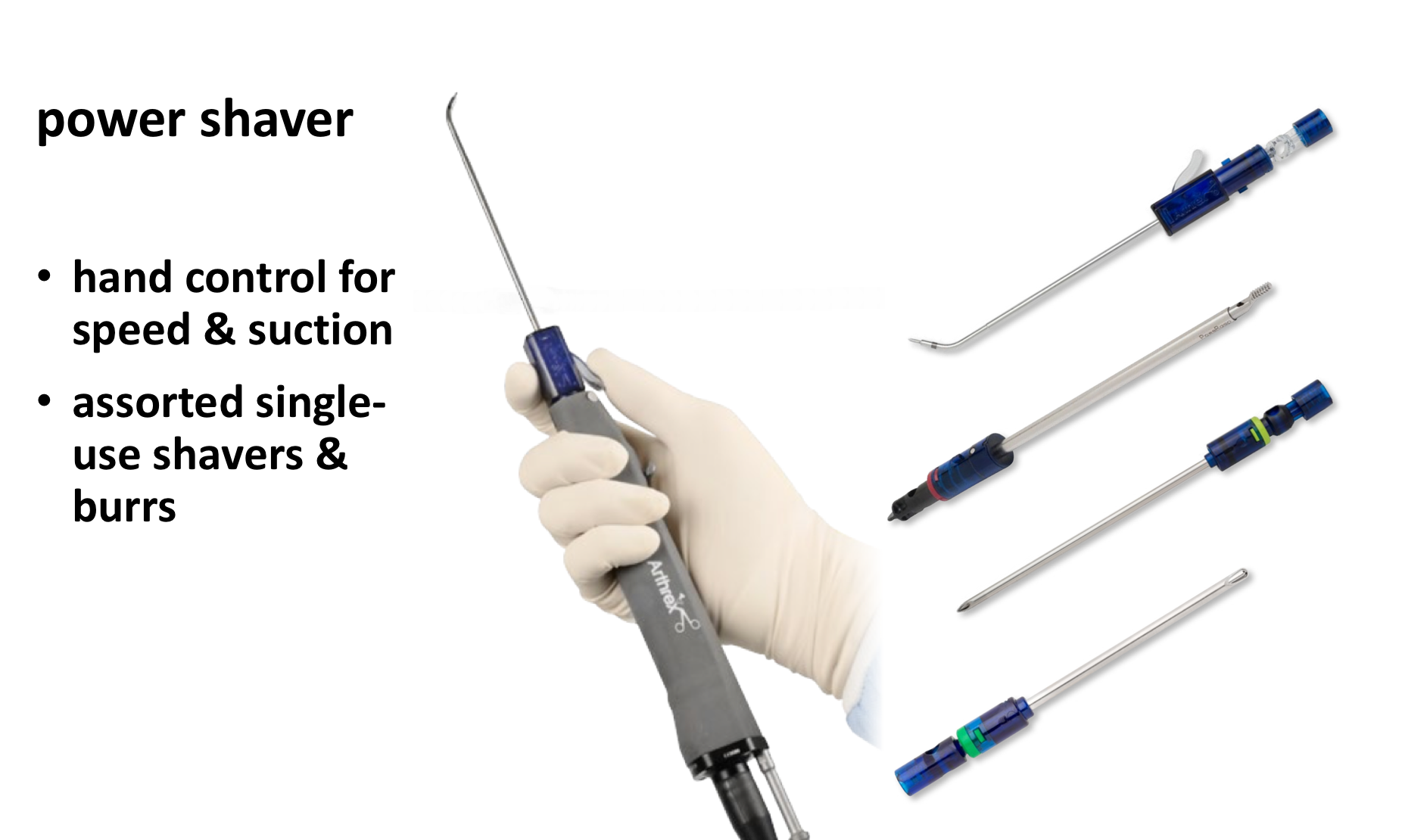
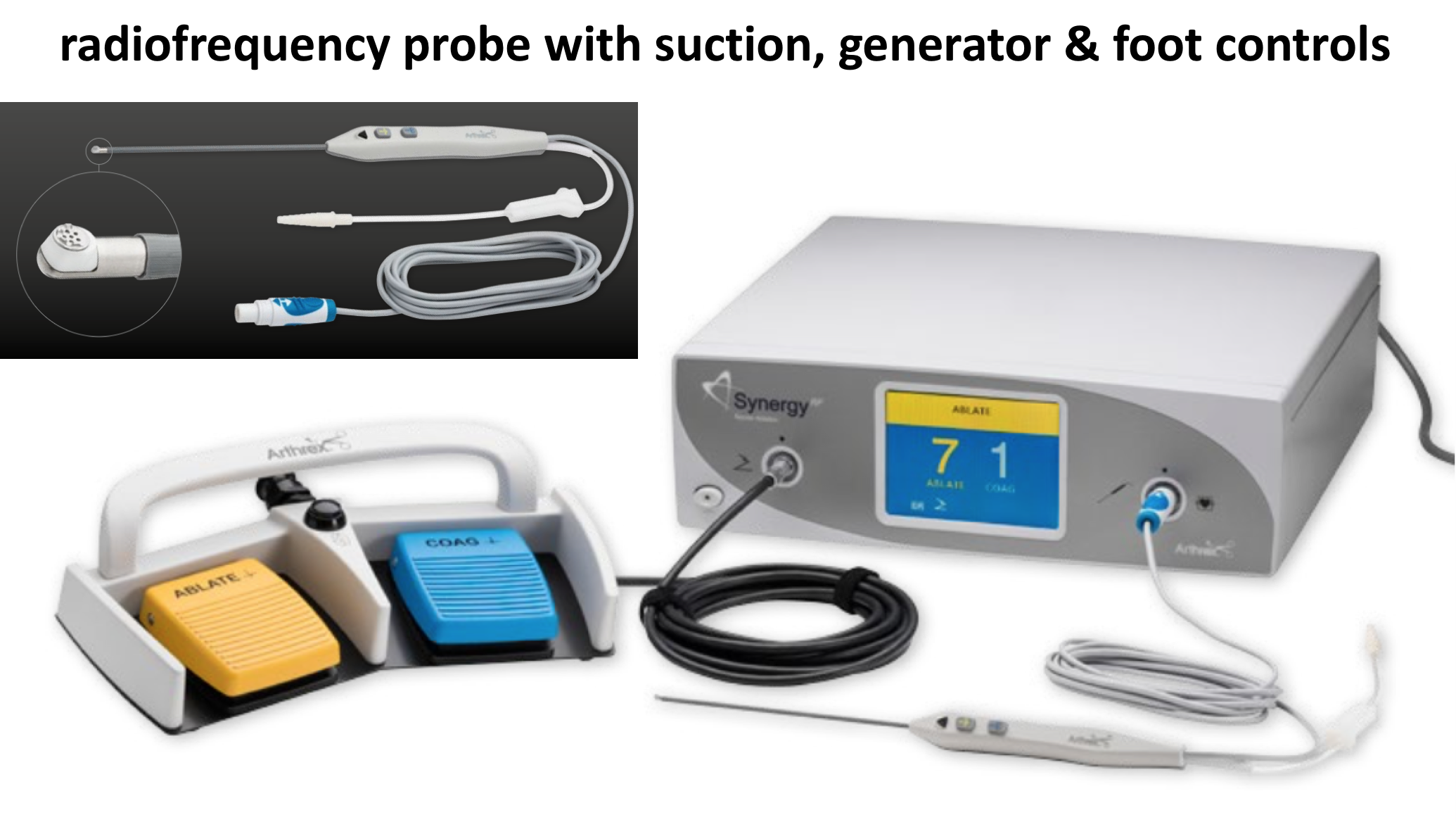
- Arthroscopic Stack – the HD Monitor, the central computer, the camera control box, pump, the light source, shaver box and radiofrequency generator are all mounted on a mobile console or stack. This can be easily wheeled in and out of the theatre and can be positioned correctly so that the surgeon can see it









Orthobiologics – PRP
Orthobiologics is an exciting new development in Orthopaedics. It is the use of natural human cells or tissue to repair or expedite the healing of an injury or a surgical repair.

- Autologous PRP (Platelet Rich Plasma) – Essentially this is the patient’s own blood plasma that has been enriched with platelets, which contain various types of cytokines and growth factors, that can potentially enhance healing.
- A sample of blood is taken from a patient and then spun in a centrifuge
- Using a number of commercially produced syringe systems the concentrated layer of the plasma, that is enriched with platelets, cytokines and growth factors, can be drawn off
- This ‘Platelet Rich Plasma’ concentrate can then be injected back into the patient into an area of injury or site of surgery
- It is postulated that this may help with the patients’ healing
- The use of PRP has expanded to many areas within medicine. However, there is little real scientific evidence that it really has a significant effect on improving healing. The best evidence is in the treatment of refractory Tennis Elbow…. find out more about PRP and Tennis Elbow
- Tendon Grafts – in certain situations where a ligament or tendon has been torn a Tendon Graft can be used to reconstruct it. This is particularly in the case of chronic injuries. Tendon Grafts are sometimes used to reconstruct and stabilise the sternoclavicular joint, the acromioclavicular joint and the elbow. The ‘donor’ tendon can be harvested from the patient (Autograft) or from a cadaver (Allograft)
- Autograft – the most commonly used Autografts are the Hamstring Tendons or Palmaris Longus. Autografts will incorporate and heal well, without the risk of infection or rejection. Harvesting these tendons does not usually lead to a functional deficit for the patient but can result in some donor site morbidity (an incision scar, initial pain and possible infection)
- Allograft – Allograft tendons come from cadavers and have undergone strict screening, denaturing and sterilization processes to avoid transfer of any infection or DNA. Allografts will not incite a rejection reaction. Allografts are expensive and do not have as good a healing potential as Autografts
- Patches – the Rotator Cuff Tendons are broad and relatively thin. There are no other tendons in the body that are this shape and so, in the case of an irreparable rotator cuff tear, no autografts are available. Allograft tendons come from adult cadavers and, as degenerative changes begin to occur at an early age, rotator cuff tendons are not of a sufficient quality to be used.
- To overcome this problem ‘Tissue Patches’, made of a collagen matrix (the essential matrix that forms a rotator cuff tendon), have been developed.
- ‘Tissue Patches’ can be made from Allograft (Human), Xenograft (Animal) or Synthetic tissues.
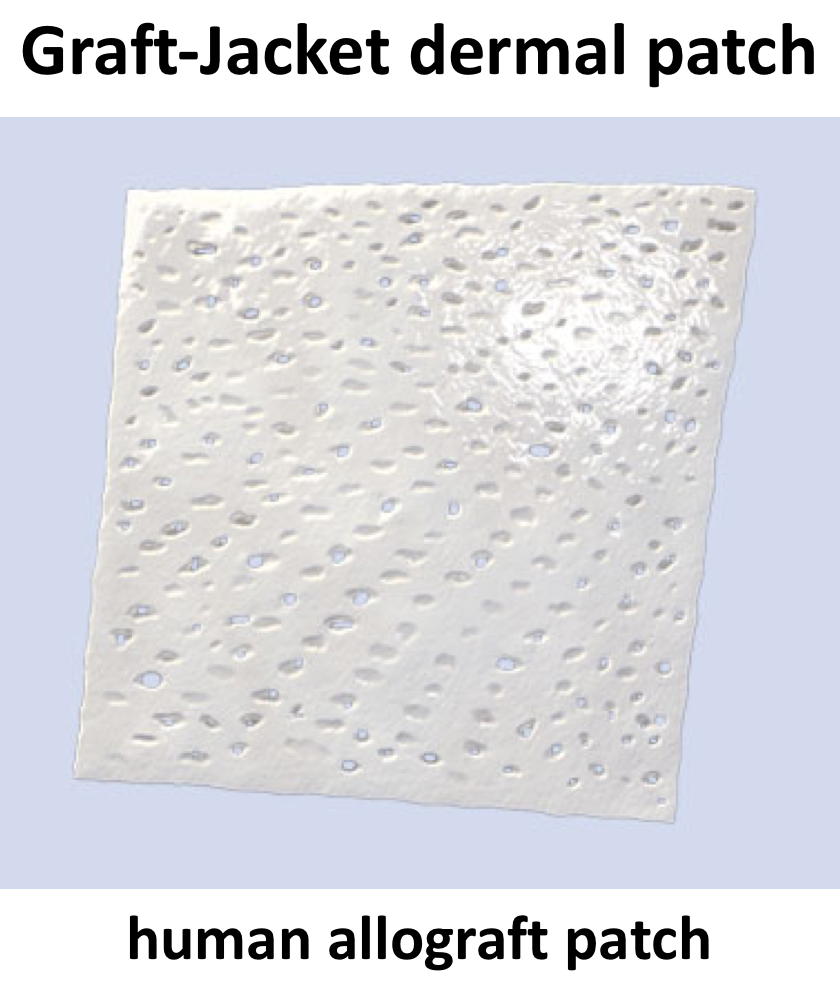
- I prefer to use Allograft (Human) patches, these are made from dermal tissue (a thick skin Graft).
- As with Allograft tendons they have undergone a strict screening, denaturing and sterilization processes. They are completely safe for human use.
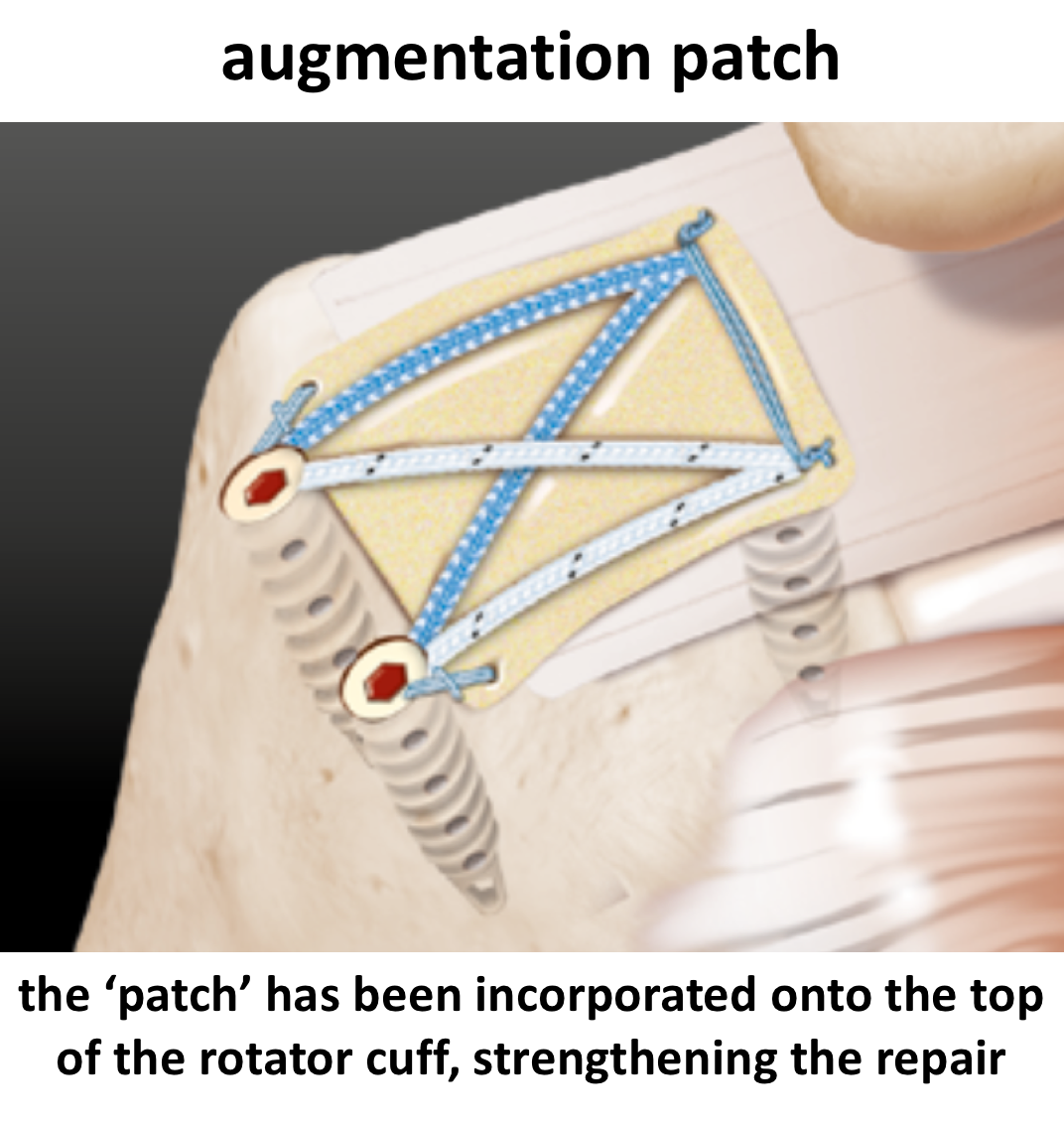
- Augmentation Patch – an augmentation patch is used on top of a rotator cuff repair where the tissue quality is poor. The patch helps to strengthen the repair.
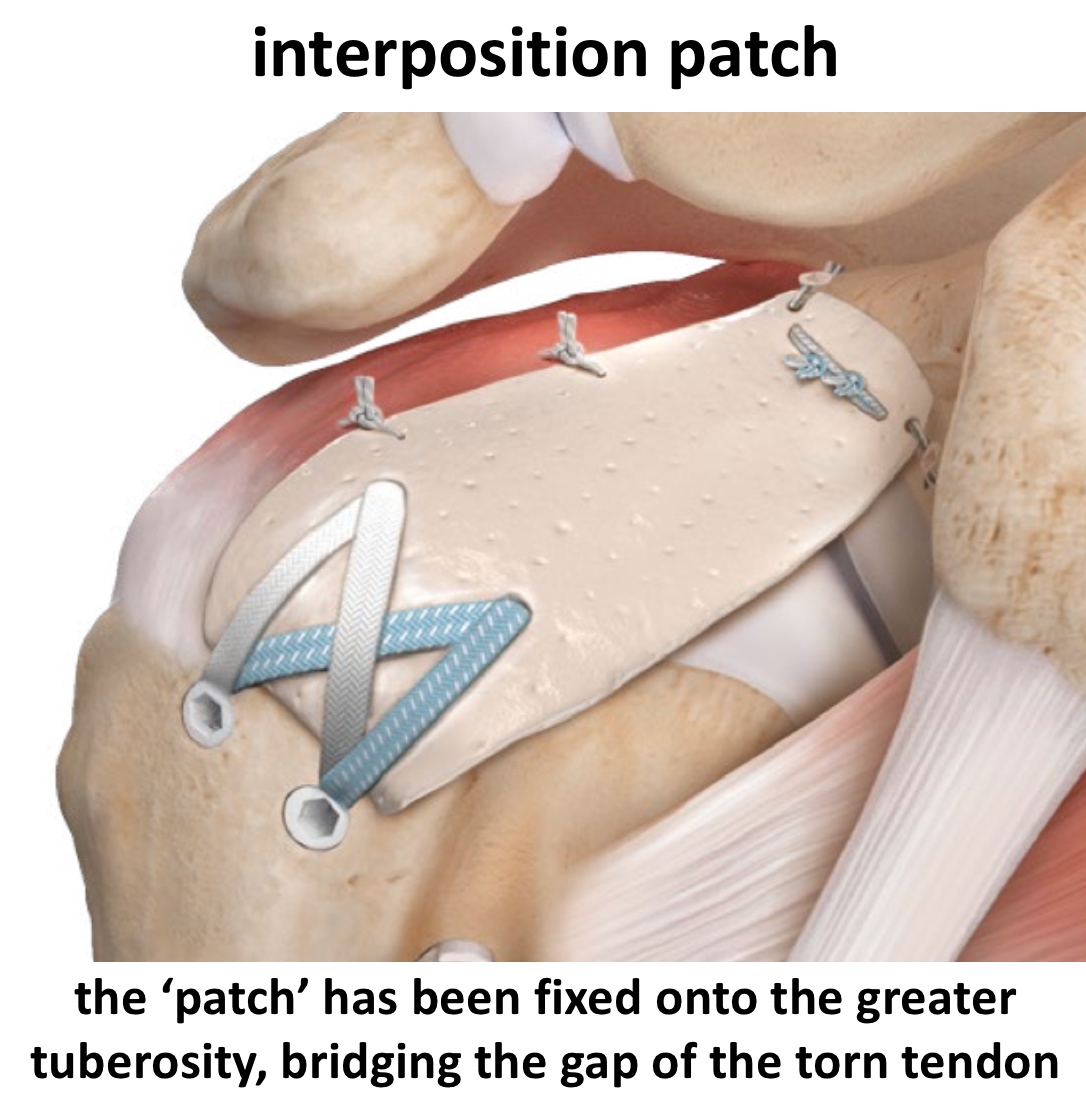
- Interposition Patch – an interposition patch is used to bridge a gap when there is insufficient tendon to actually make a repair.