






Arthroscopic Bankart Repair (Anterior Shoulder Stabilisation)
A Bankart Repair operation can be undertaken as an open or an arthroscopic procedure. The advantages of an arthroscopic procedure are that smaller incisions are used without having to disturb and cut through other structures and it is possible to more accurately assess the damage to the shoulder and quality of repair.
I undertake all of my Bankart Repairs arthroscopically. There are a number of different variations to the technique and different implants that can be used. I have evolved my technique over the past 15 years, taking advantage of new implants and equipment, and have obtained consistently good results, with which I am happy. My routine Arthroscopic Bankart Repair is described below,


Watch a video of an arthroscopic Bankart Repair….
Find out more about Arthroscopic Shoulder Surgery….
Procedure
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block…. - Prophylactic iv antibiotics are given
- A posterior and 2 anterior portals are used for joint access
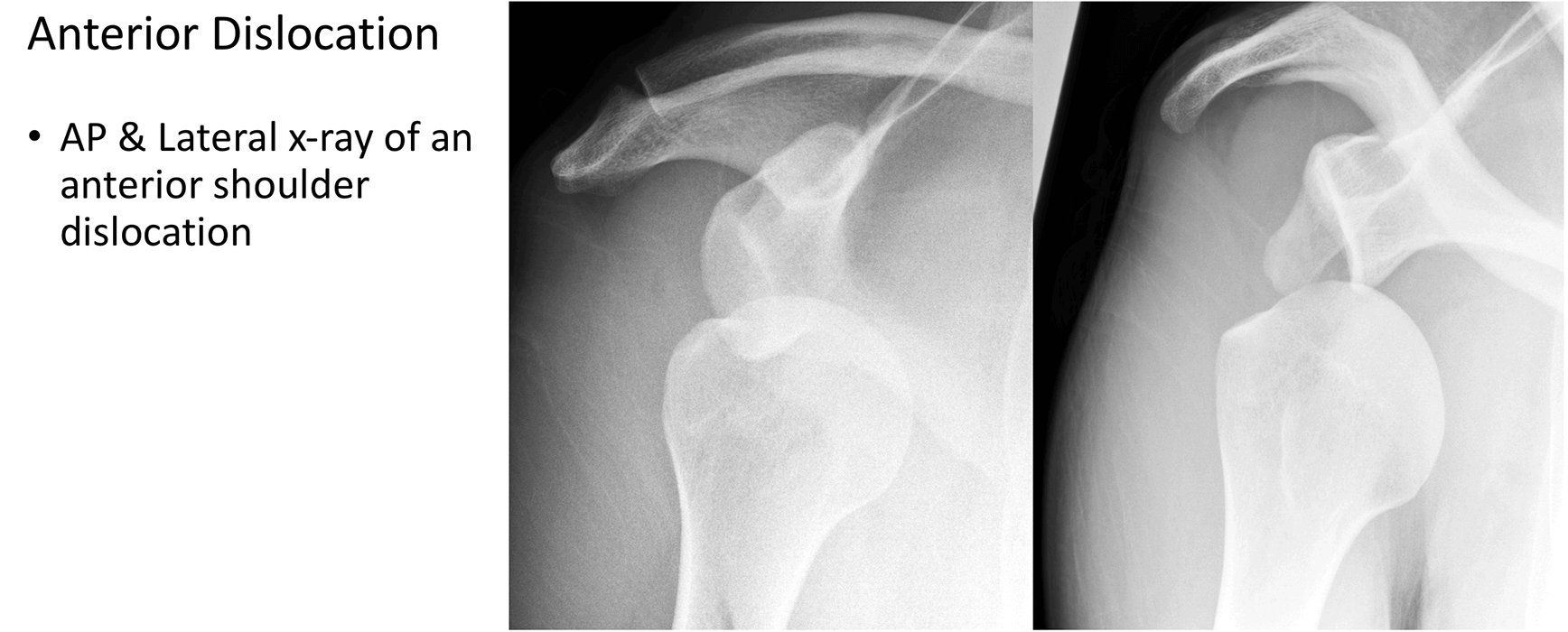
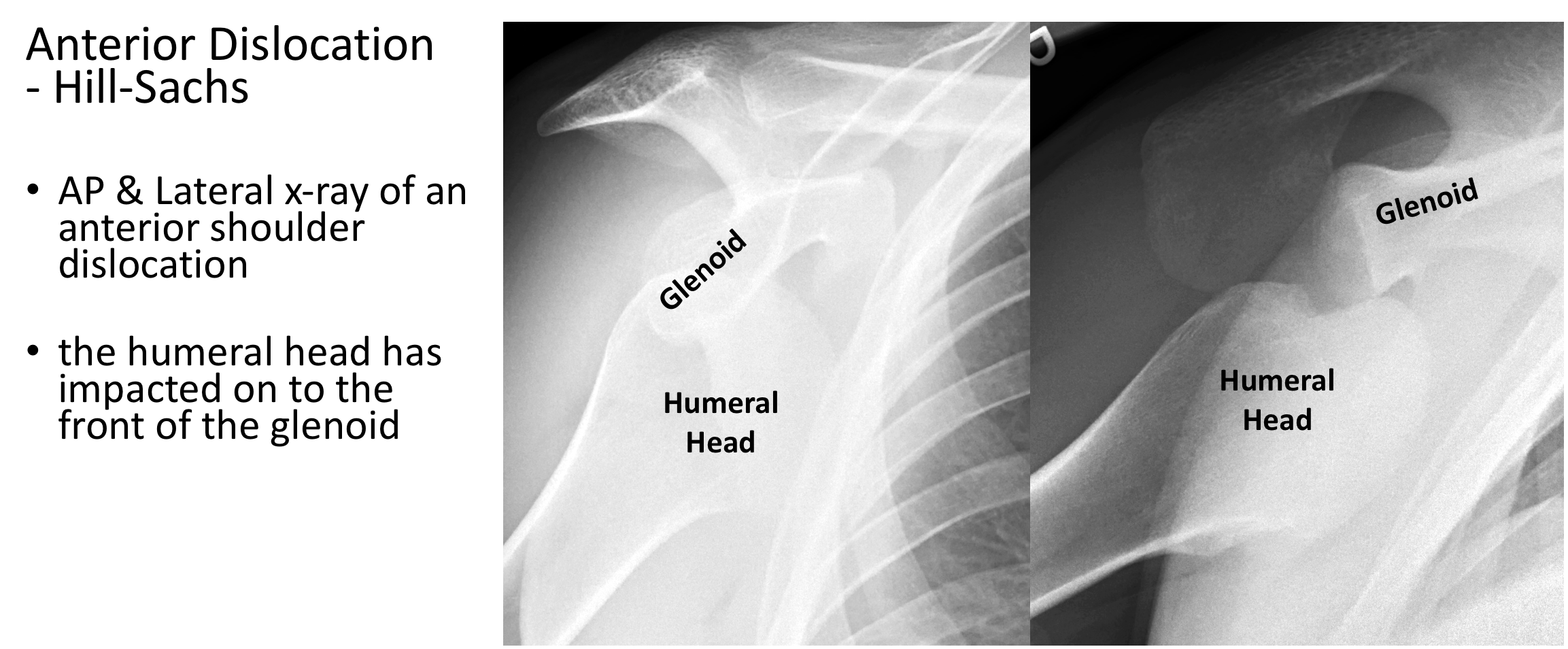
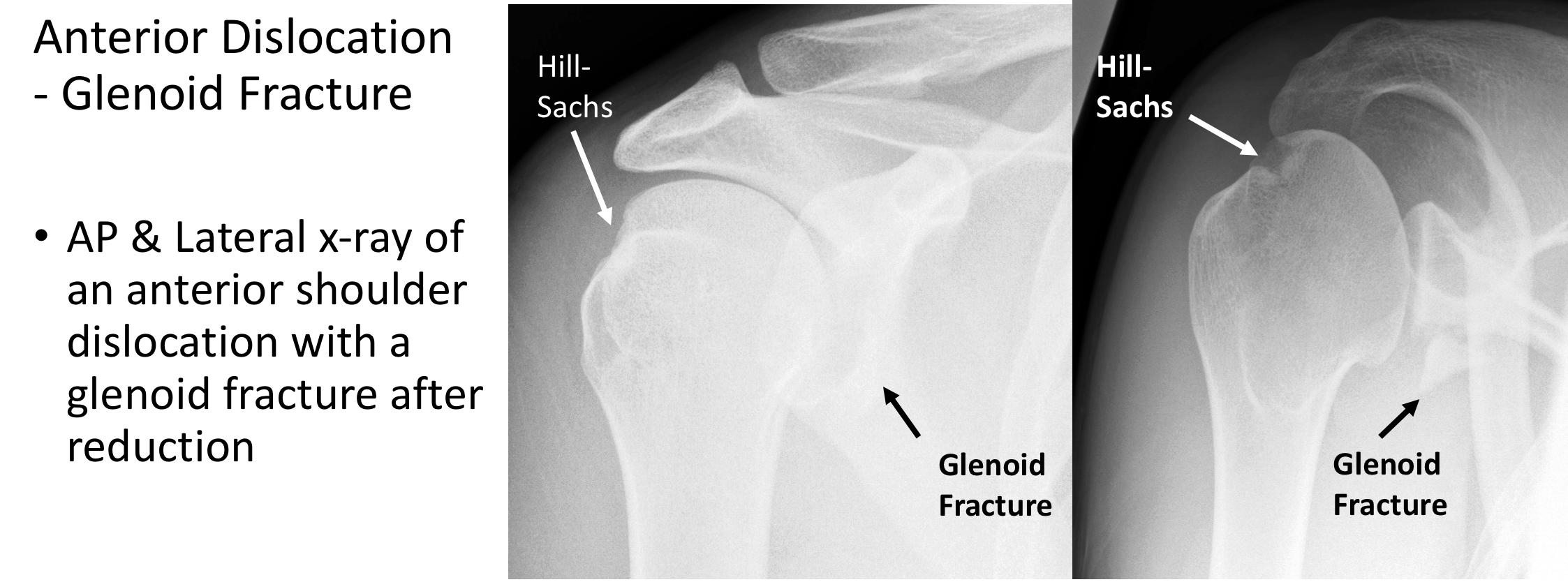
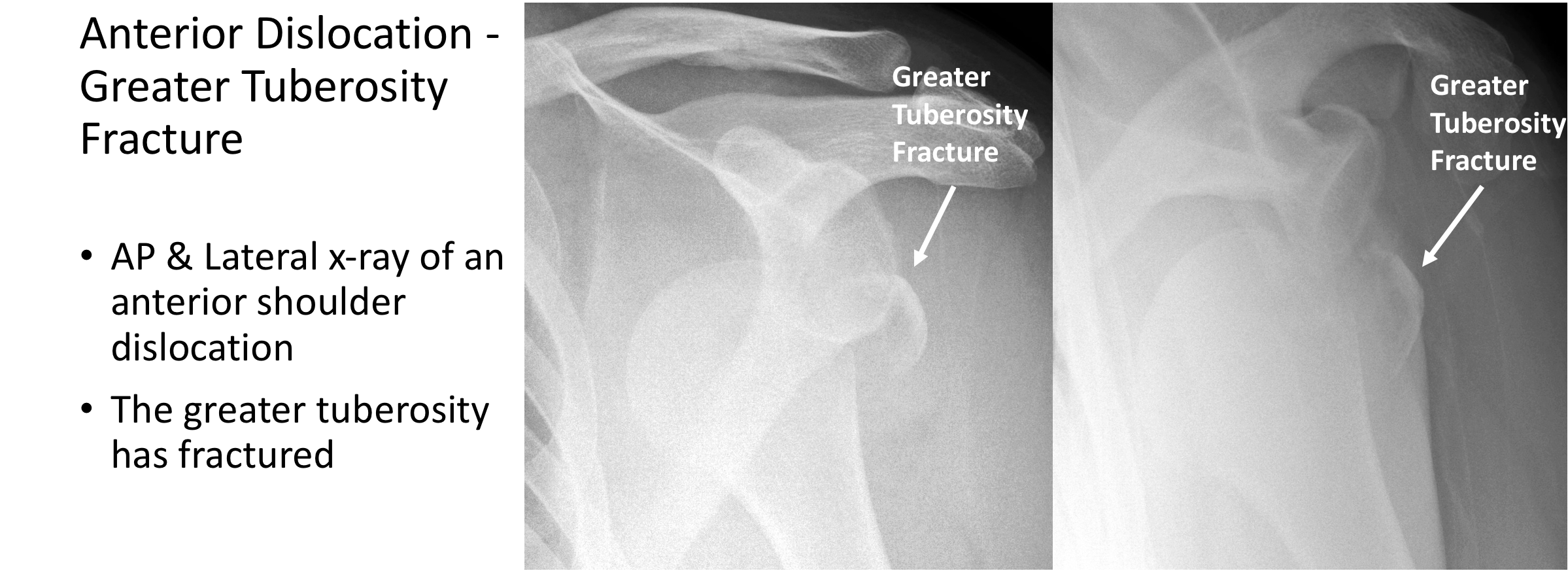
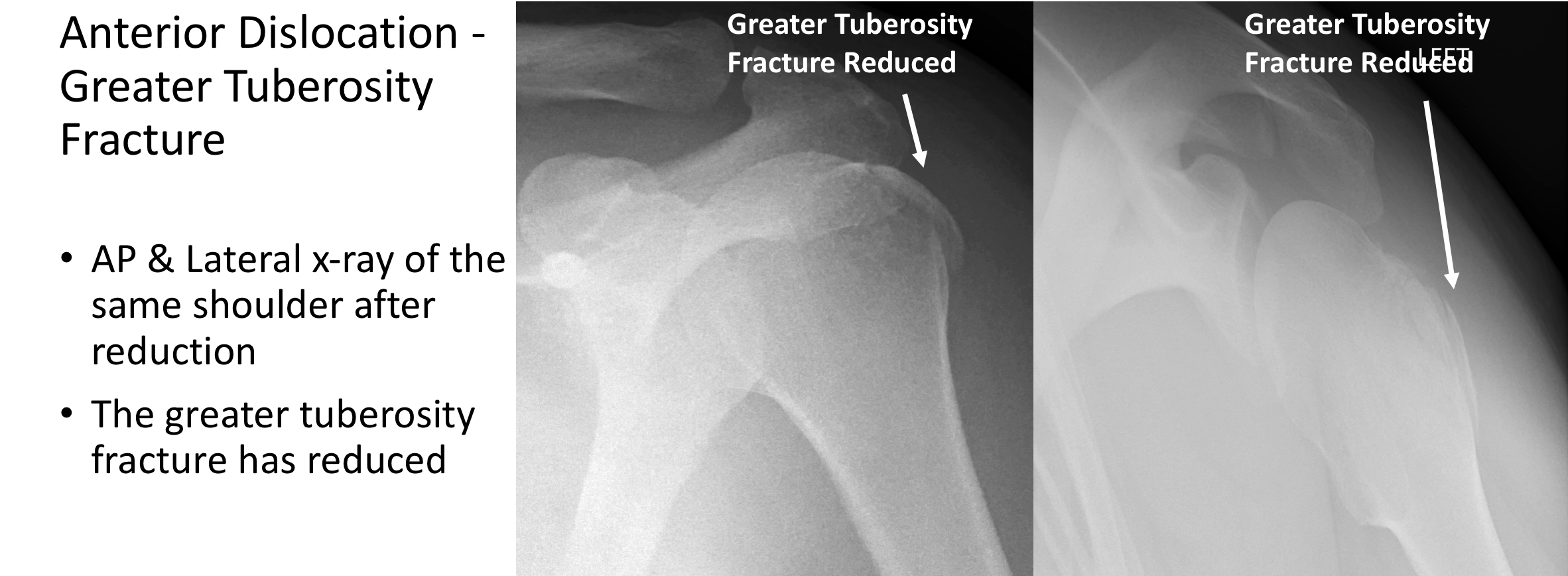
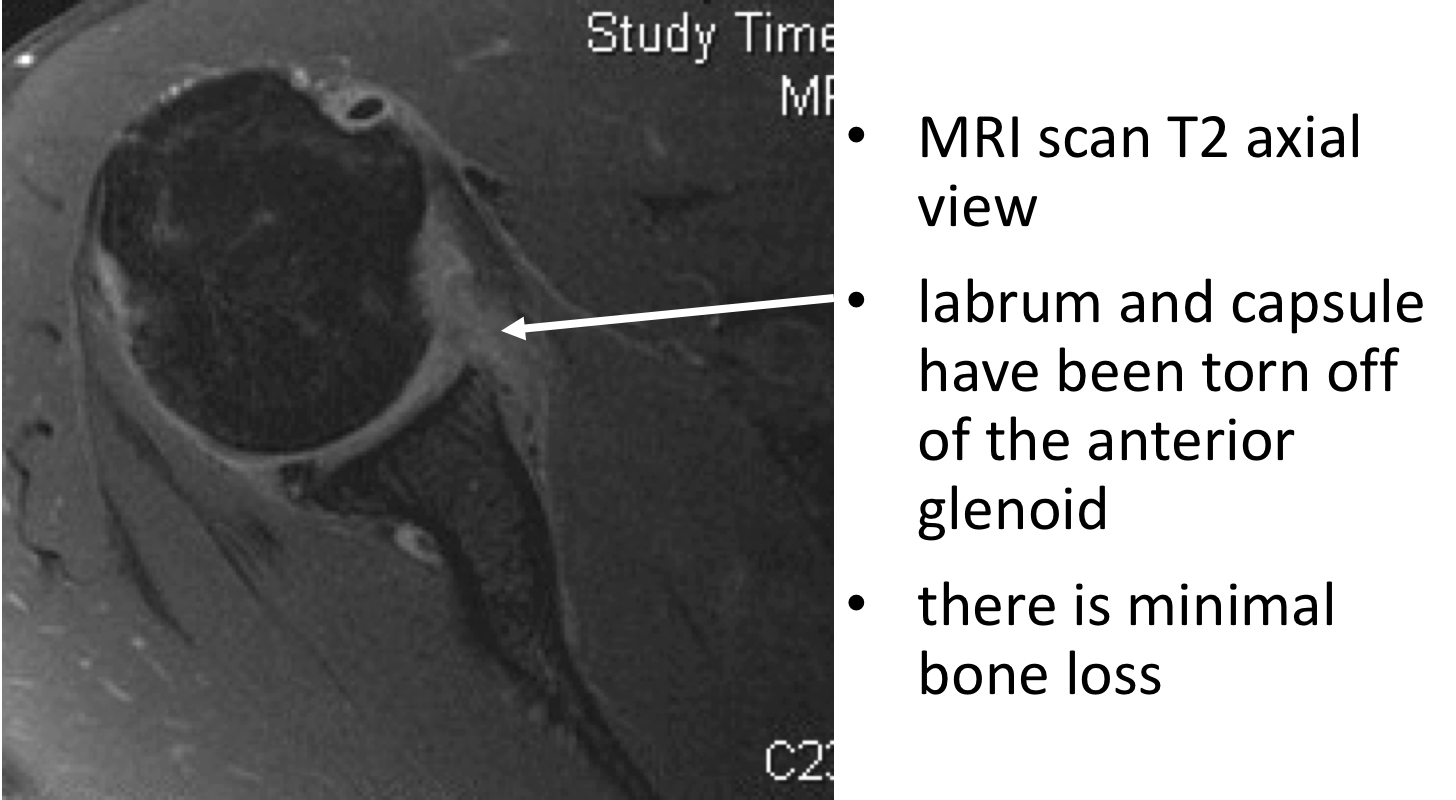
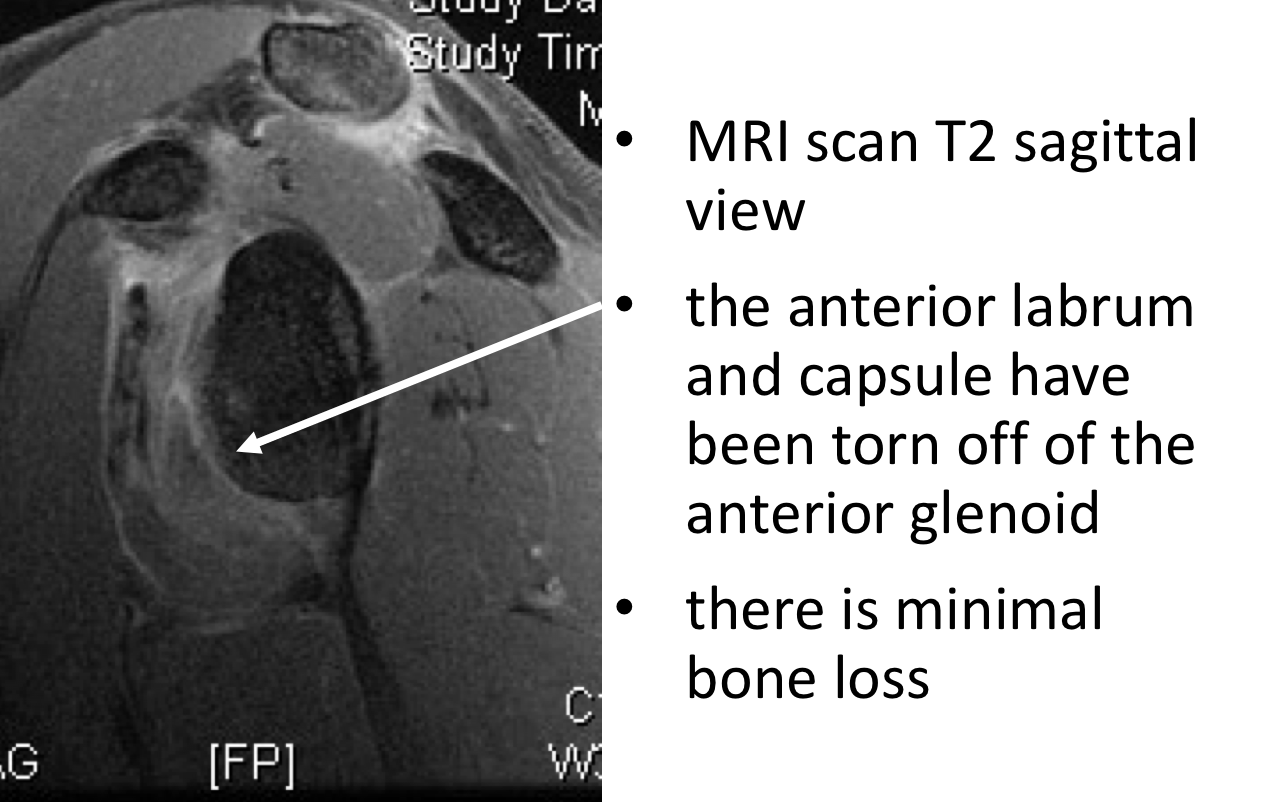
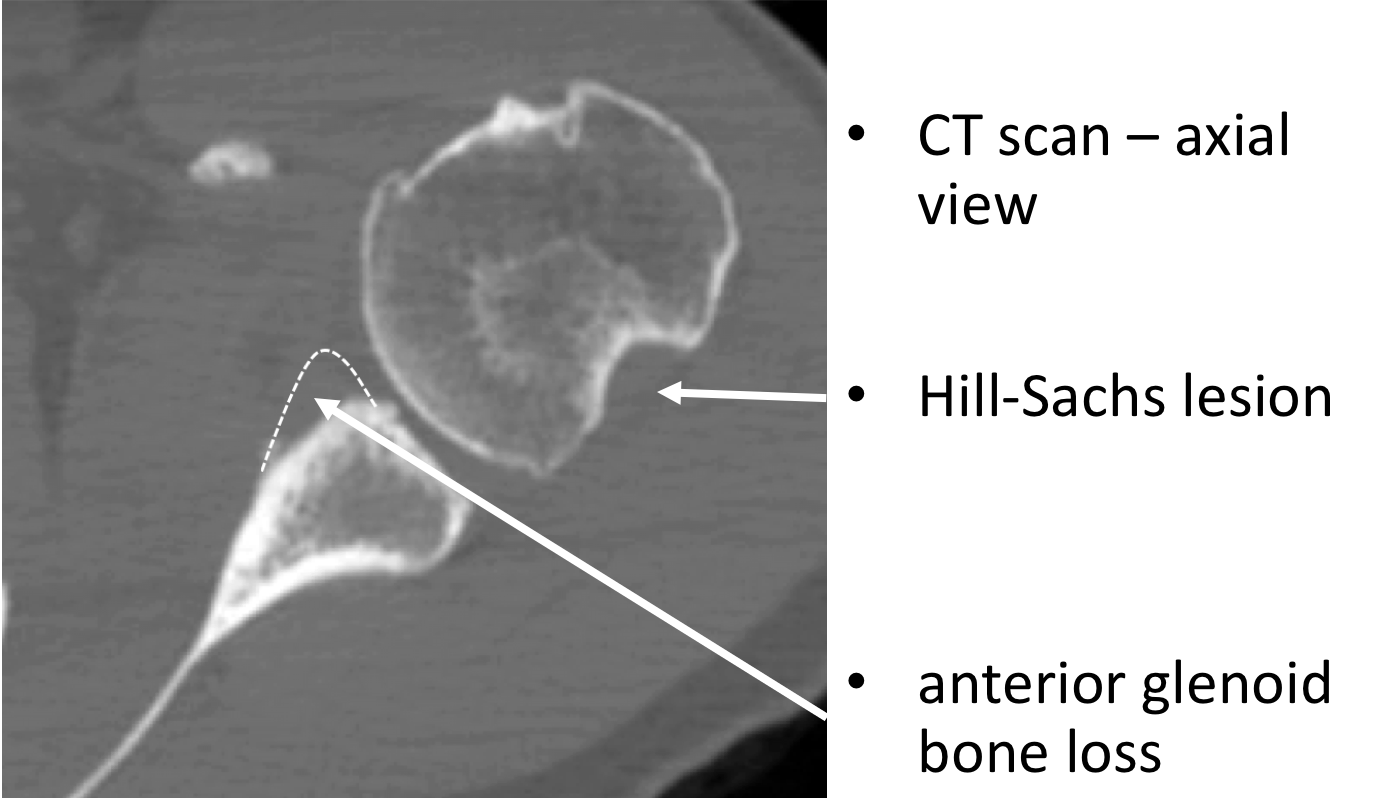
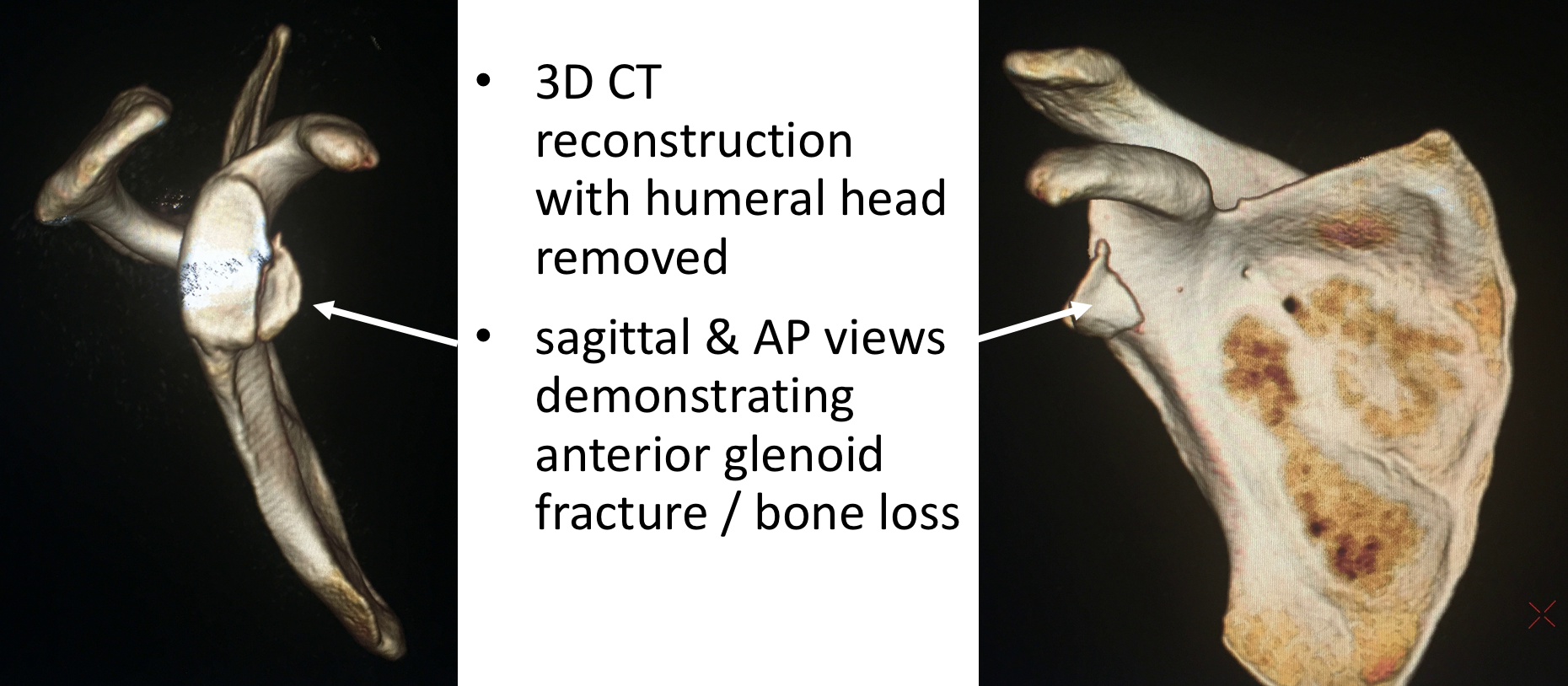
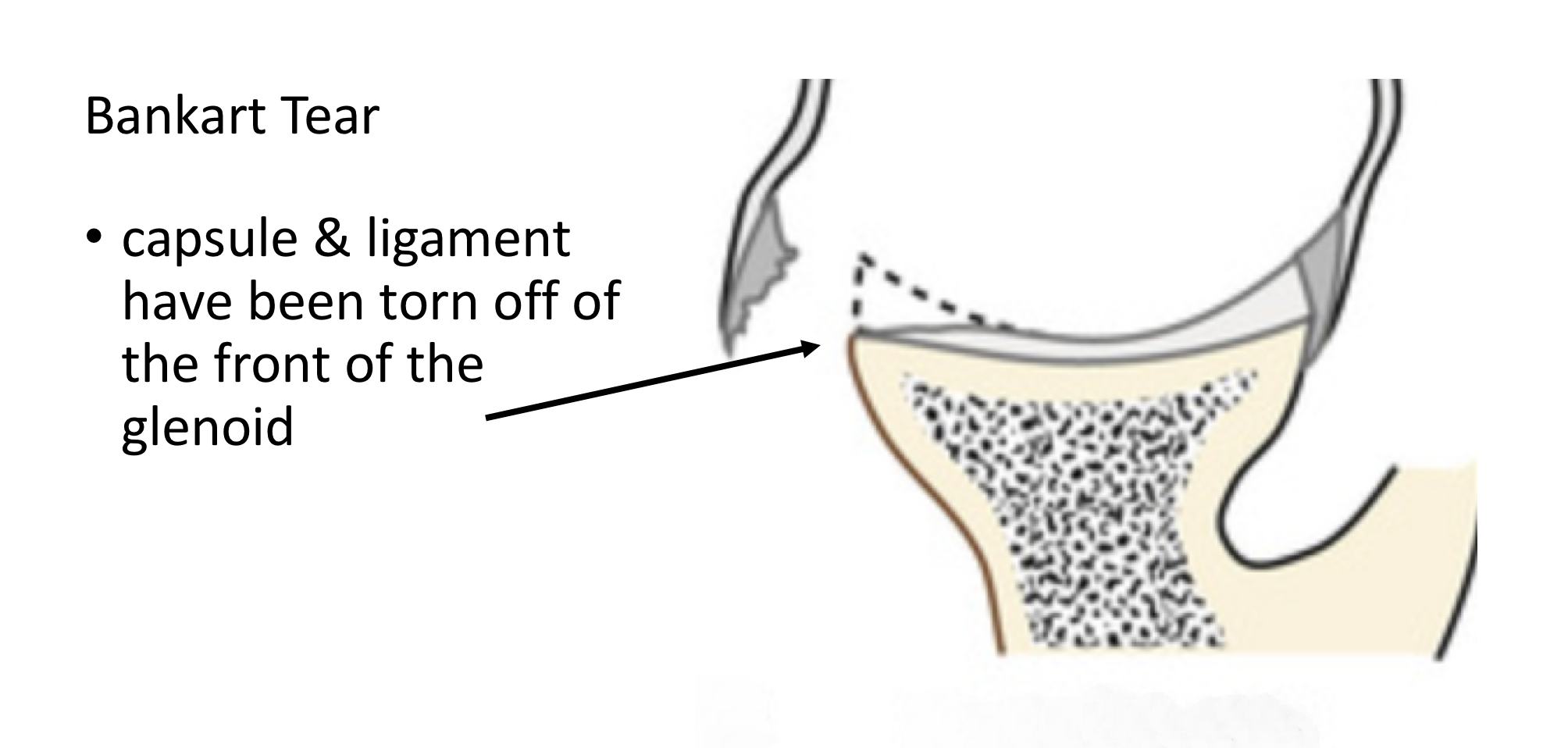
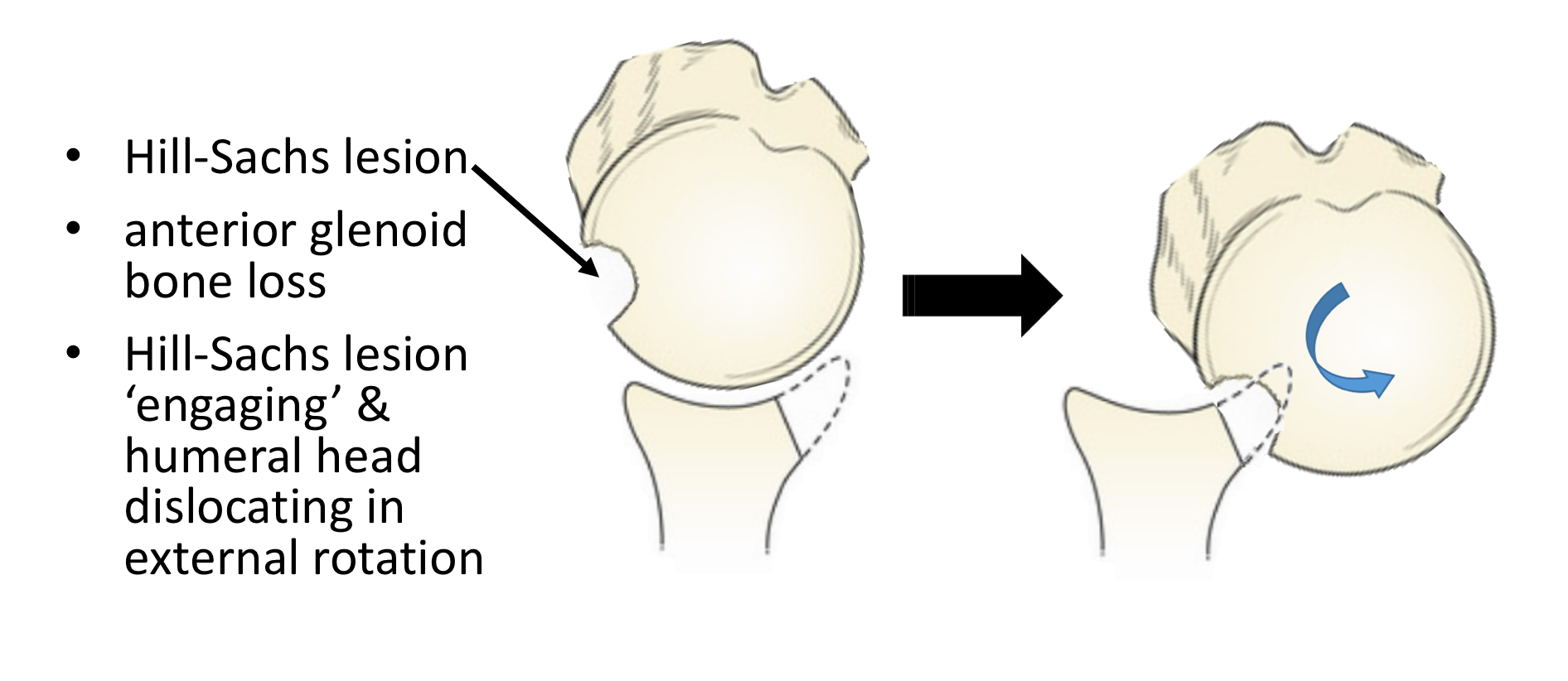
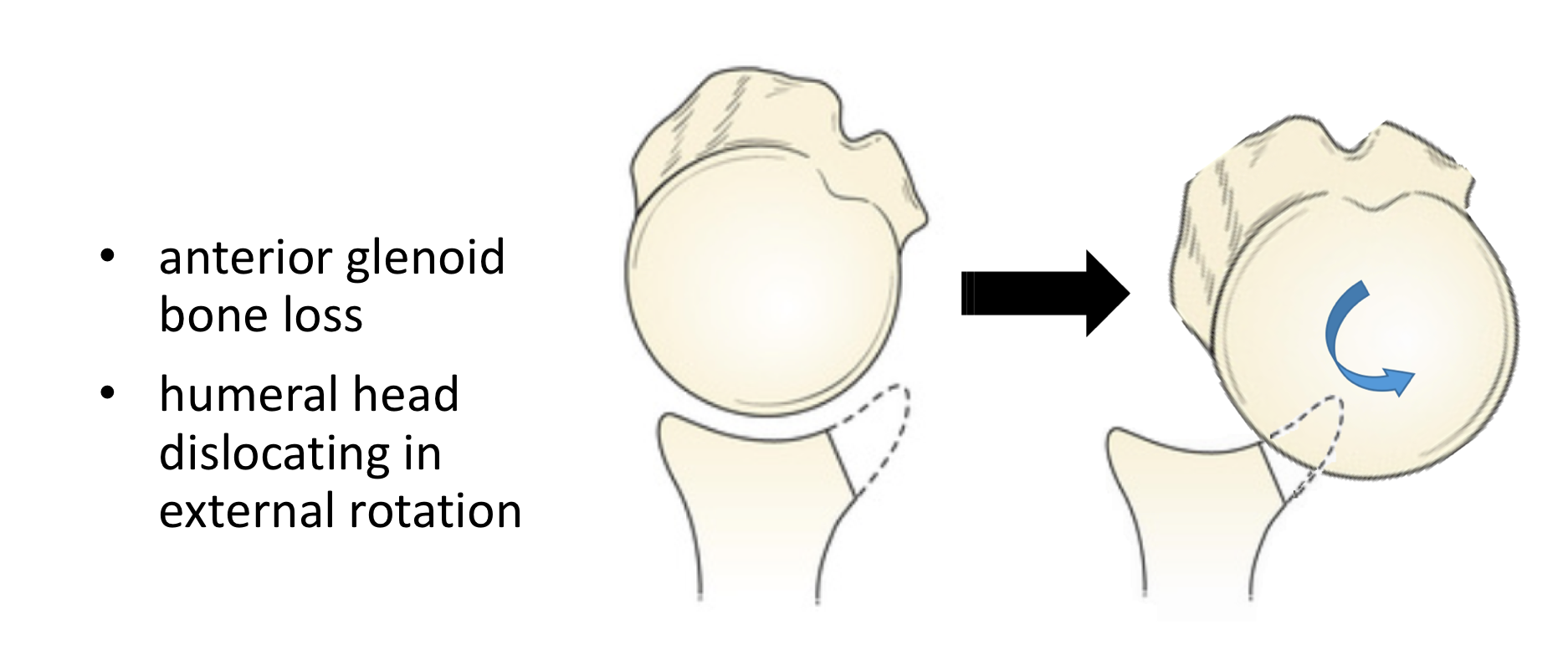
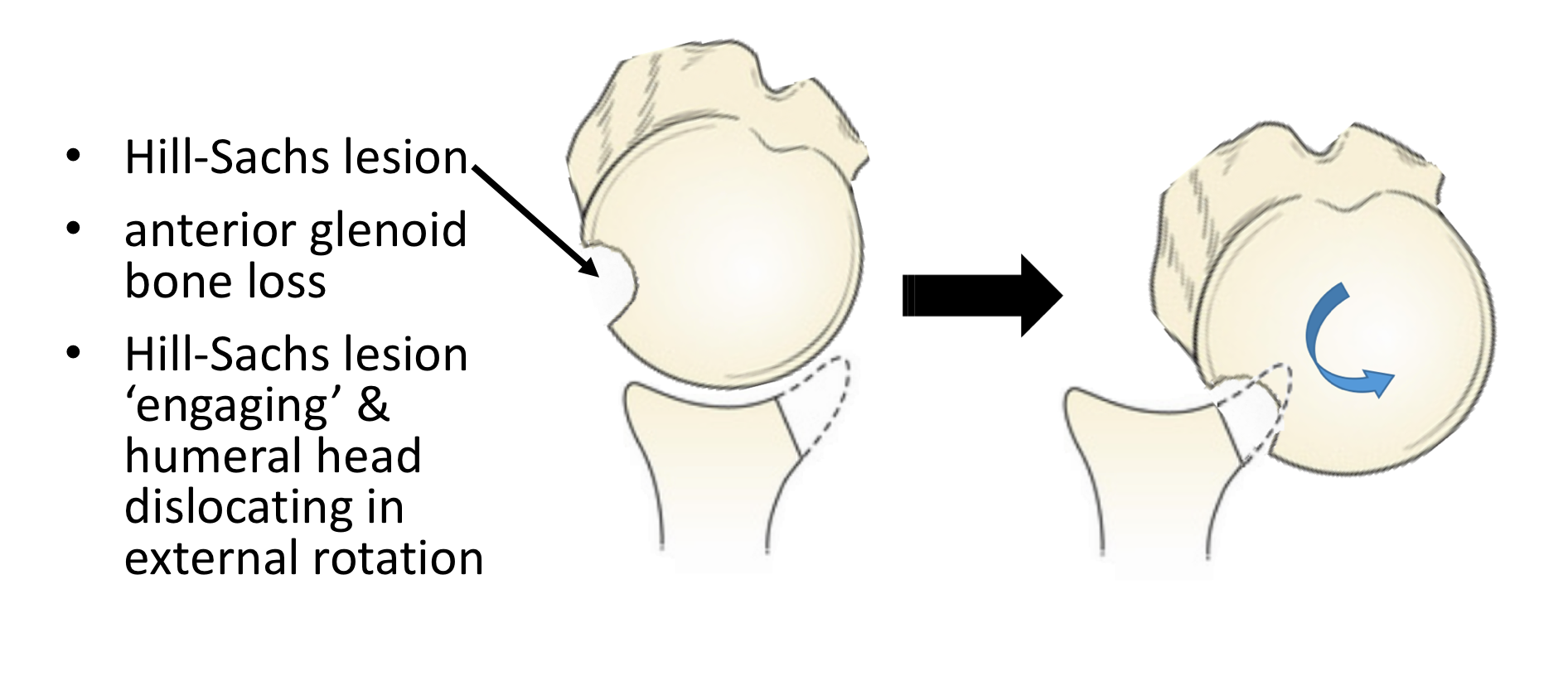
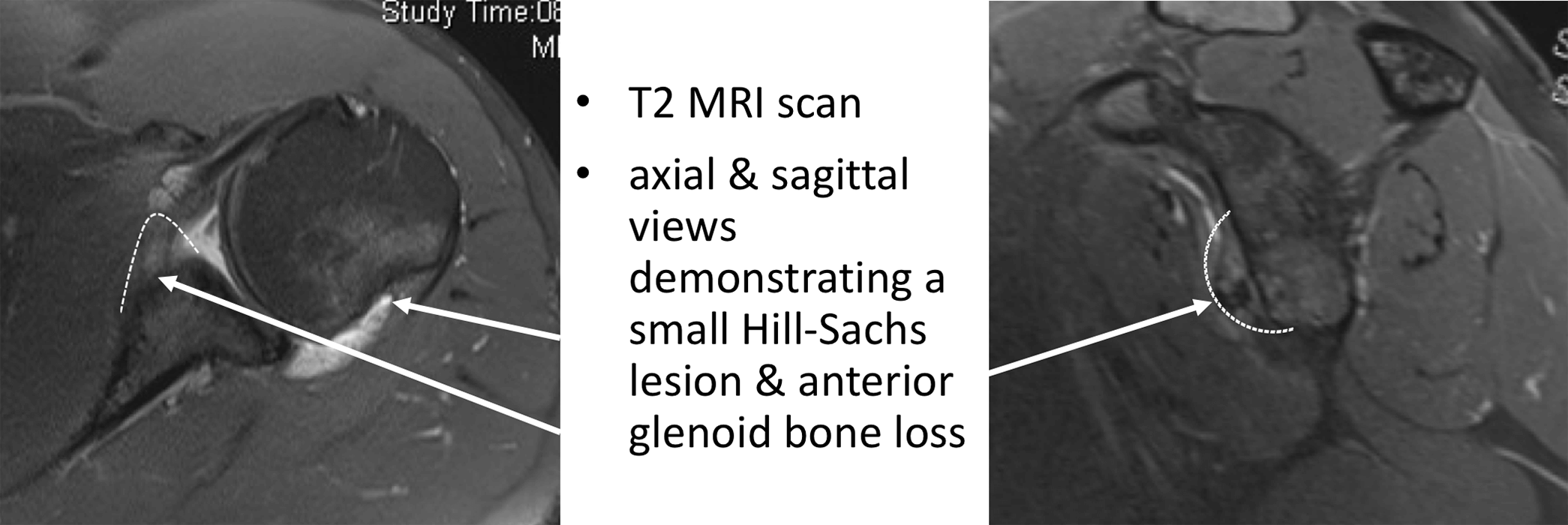
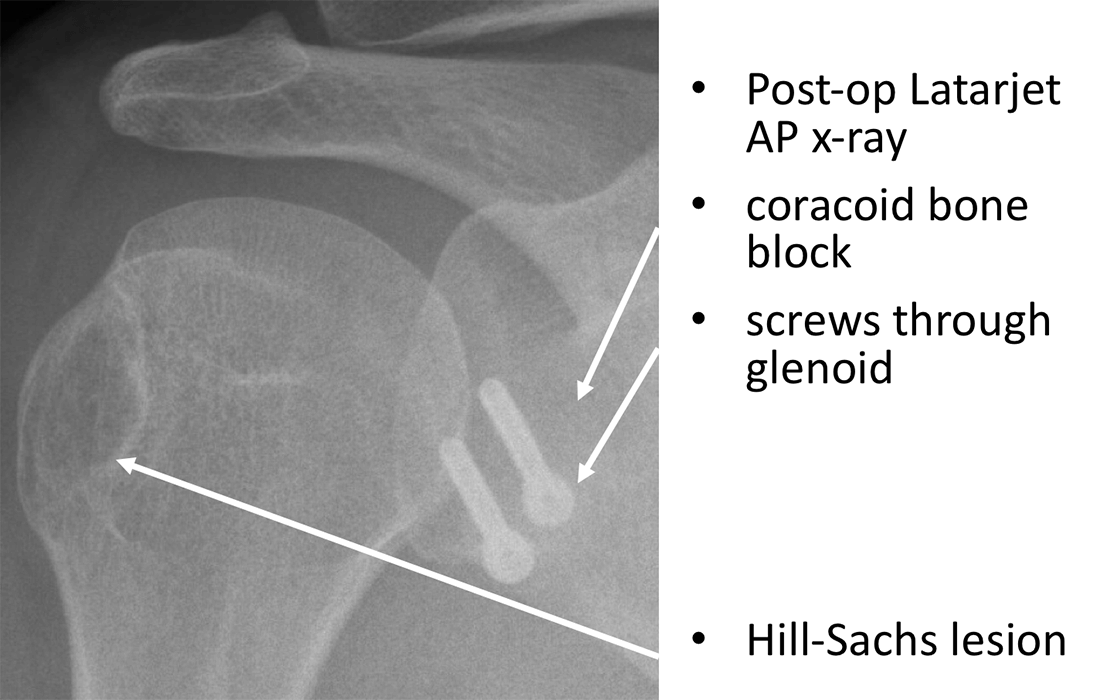
- The joint is initially assessed to confirm the presence of the Bankart Tear, to assess the extent of any Hill-Sachs Lesion or Glenoid Bone Loss and any other pathology
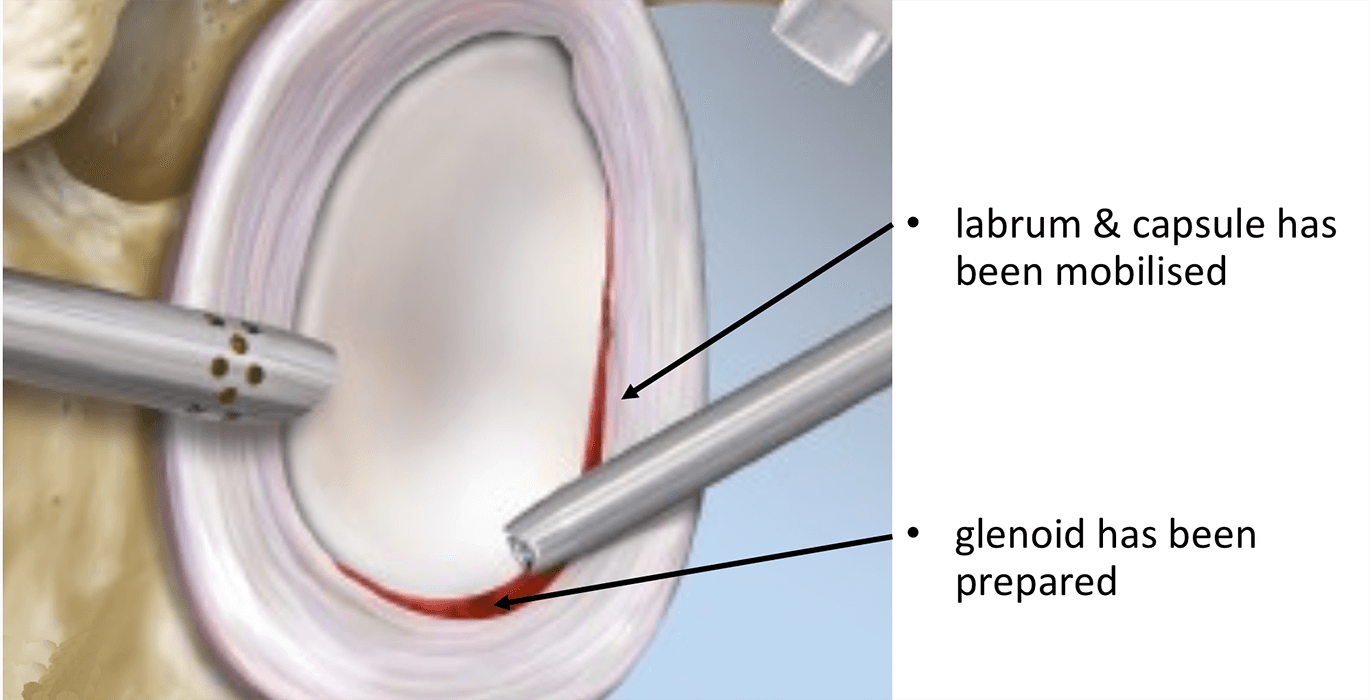
- The Bankart Tear is then fully mobilised and the tissues freshened
- The Anterior Glenoid is then prepared and freshened
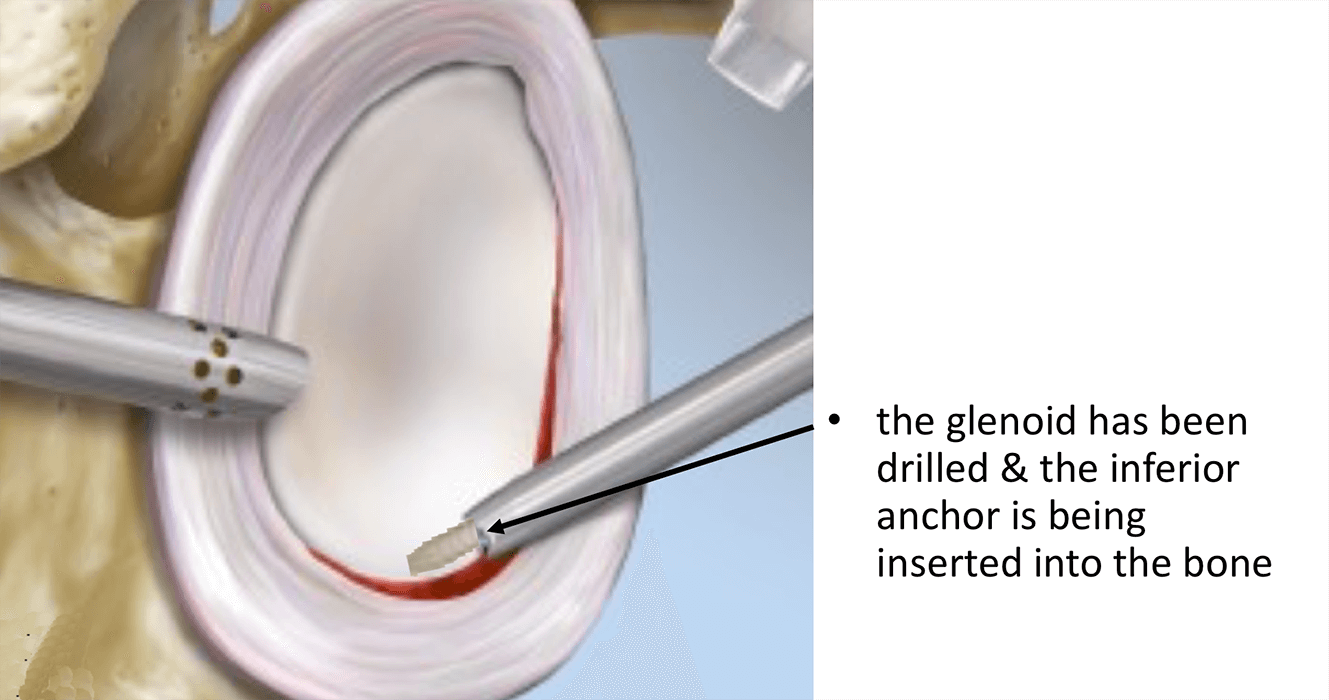
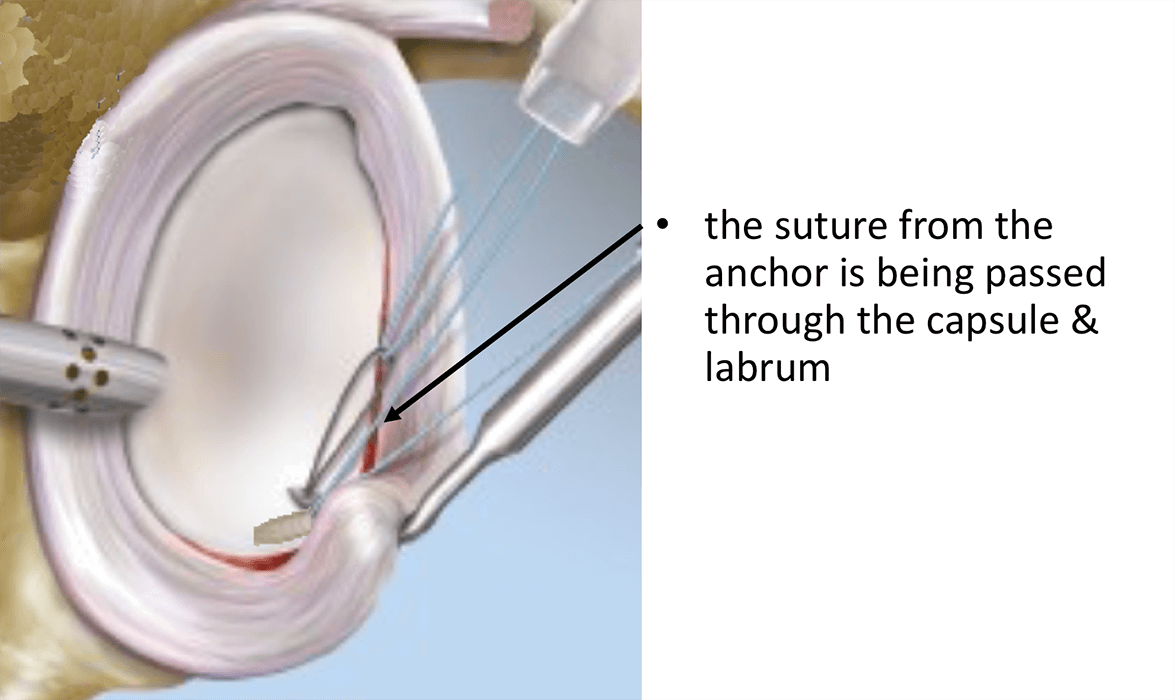
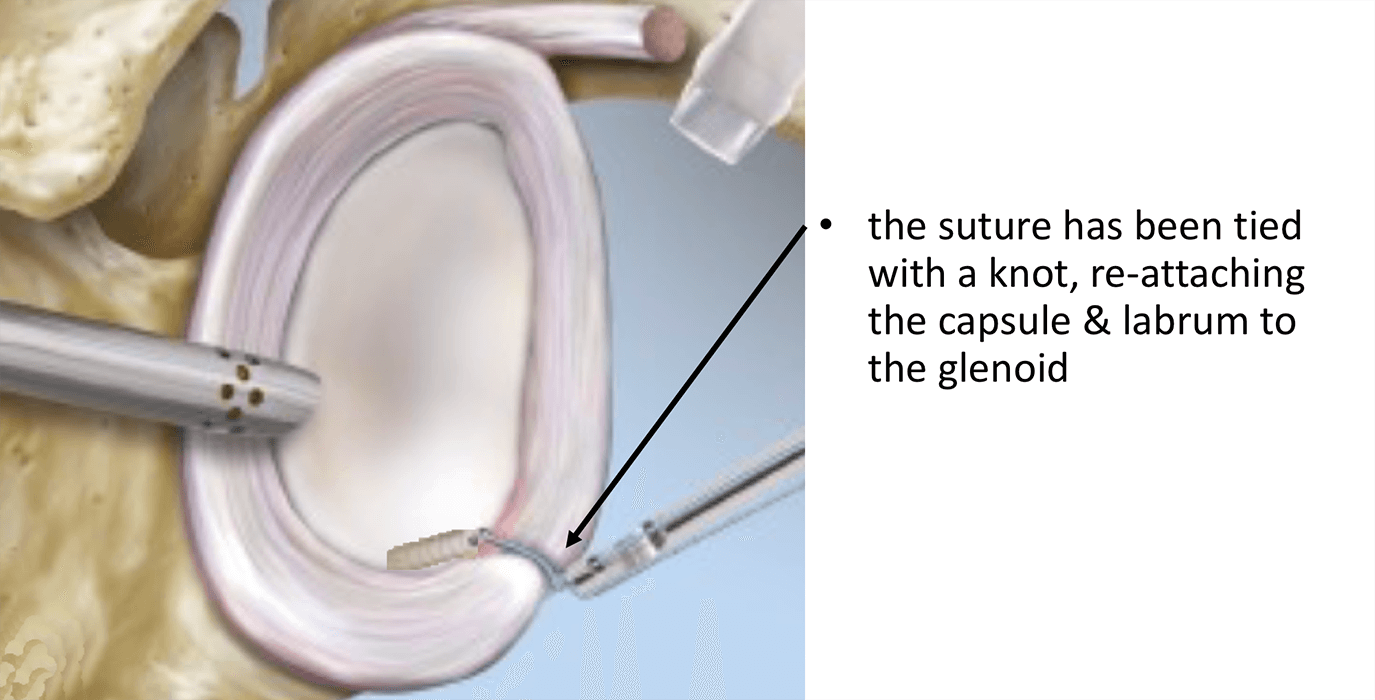
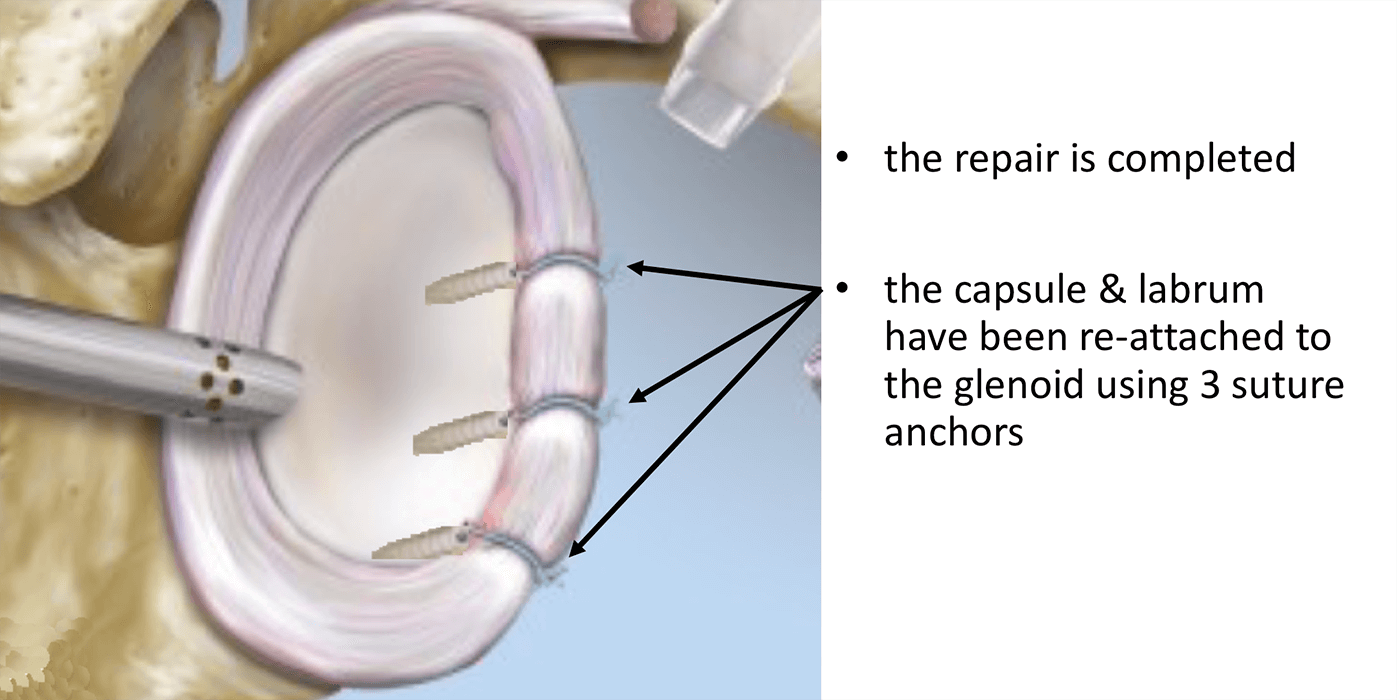
- 3 Osteoraptor or Pushlok bio-composite anchors are inserted into the anterior, inferior glenoid and the capsule and ligaments re-attached with a superior shift
- The repair is assessed and the wounds closed


This is my procedure of choice to treat Anterior Shoulder Instability with significant Bone Loss. It is an operation that I am able to undertake as both an Open and Arthroscopic procedure.


Watch a video of an arthroscopic Latarjet procedure….
Find out more about Arthroscopic Shoulder Surgery….
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
Anterior Bone Block Procedure (Eden-Hybinette Procedure)
The standard Eden-Hybinette uses a 1.5 – 2cm tri-cortical Bone Graft that is harvested from the Iliac Crest, which is the bone at the front of the hip. This is done through a 5cm incision just above the crest and, although sometimes painful for a time afterwards, does not usually lead to any detrimental function. The Bone Graft is then prepared with 2 drill holes.
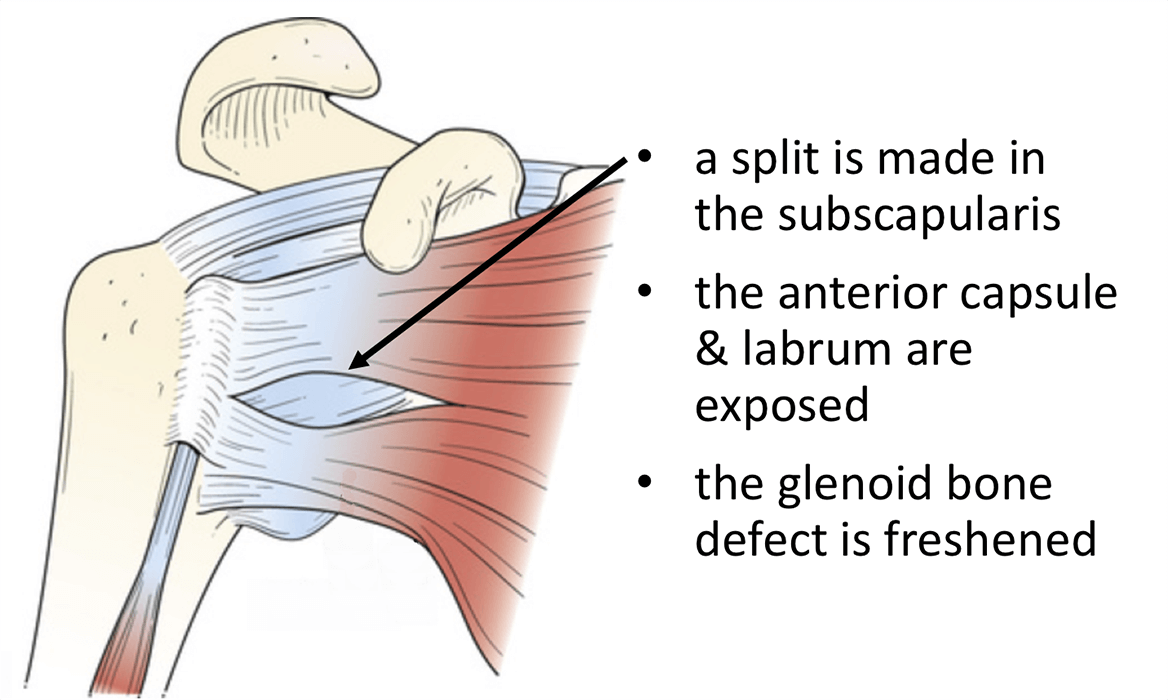
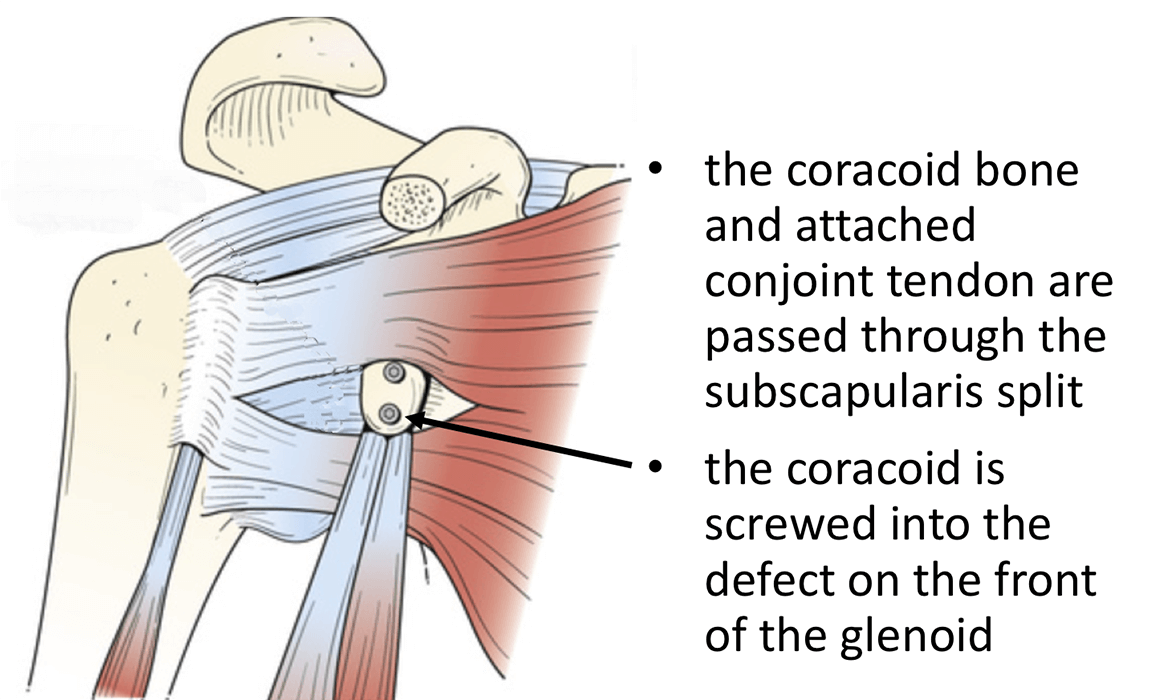
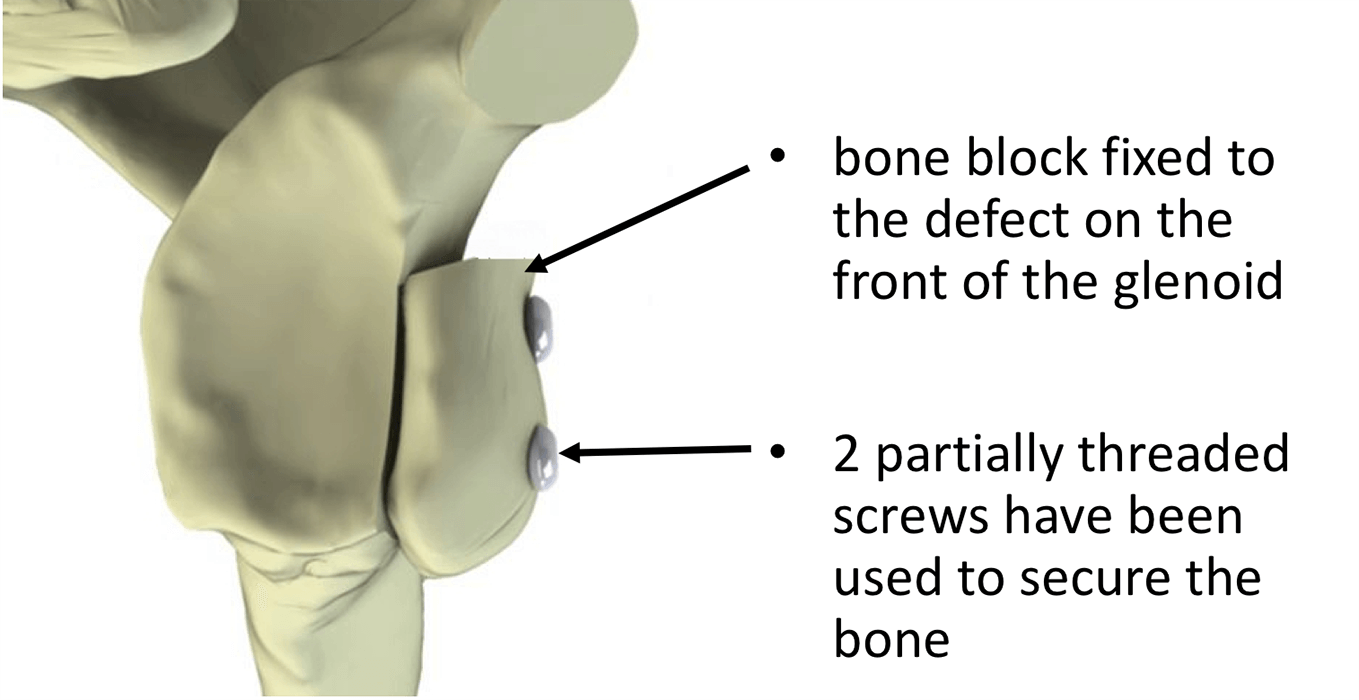
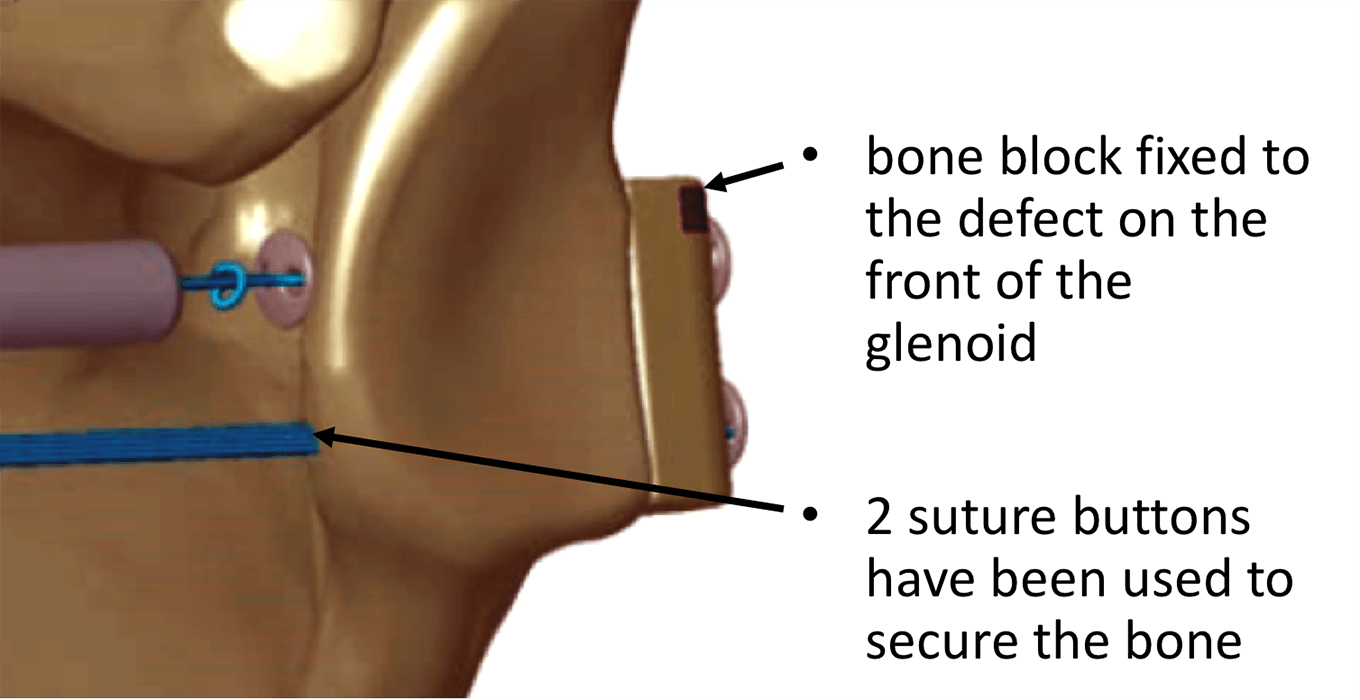
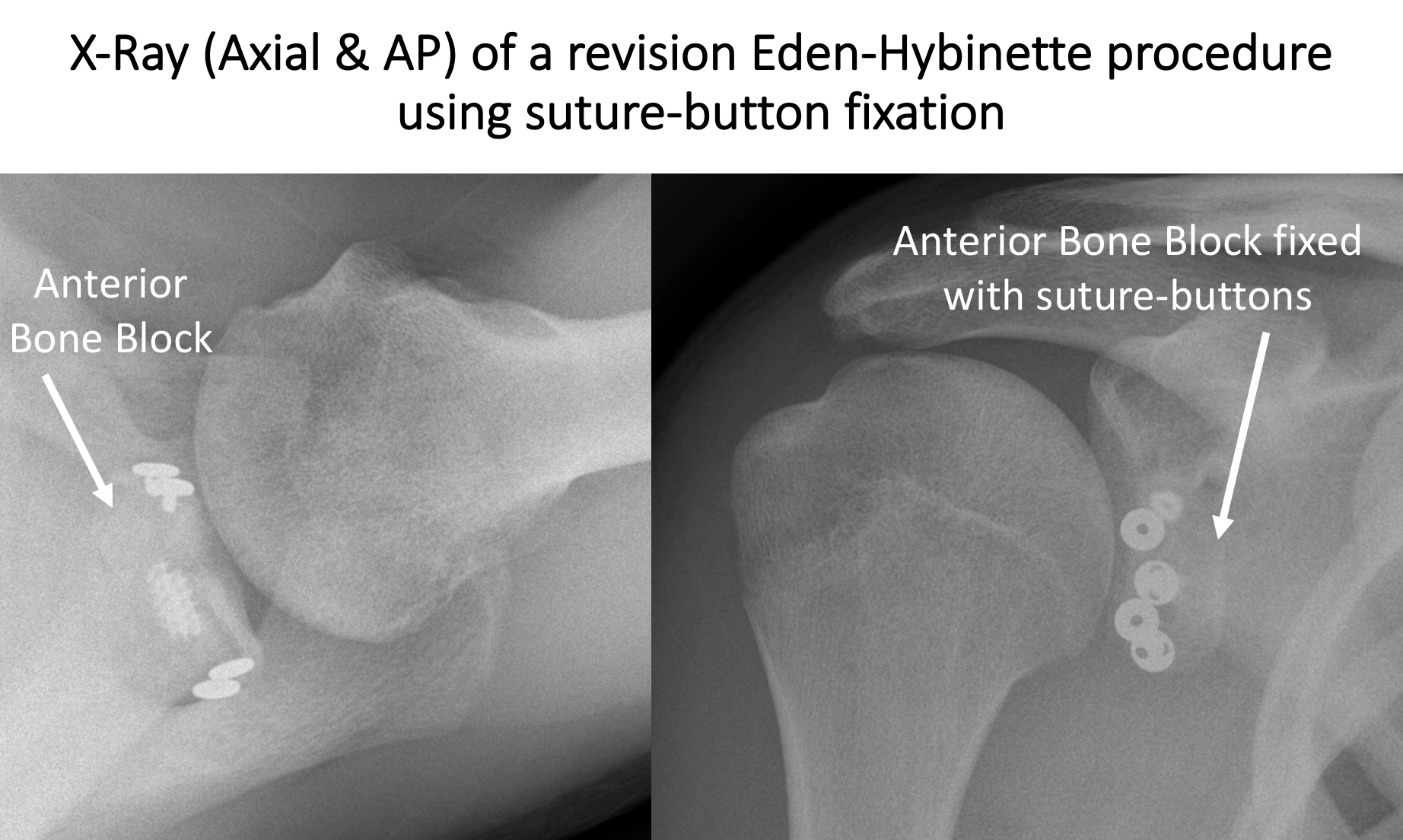
The front of the shoulder is then approached and, by either splitting the Subscapularis Tendon along the line of its fibres or by retracting the top edge of it downwards, the front of the Glenoid exposed. The area of the Glenoid defect is then prepared and the pre-prepared Bone Graft positioned over it. Through the prepared drill holes in the Bone Graft the Glenoid is drilled and 2 screws are inserted fixing the Bone Graft onto the front of the Glenoid. Various types of screws and suture-button devices can be used to do this. The joint capsule and ligaments are sometimes then re-attached to the glenoid, depending on their condition.
The advantage of the Eden-Hybinette procedure is that none of the other structures around the shoulder are disturbed and it recreates the near normal anatomy. The disadvantages of the procedure are that it requires a donor site at the hip, there is often a loss of 5 – 10 degrees of External Rotation and that it does not provide the additional ‘Dynamic Sling’ effect that the Latarjet procedure offers.
Watch a video of an arthroscopic Eden-Hybinette procedure….
Watch a video of an arthroscopic Eden-Hybinette procedure….
Find out more about having an anaesthetic….
Find out more about an Inter-scaelene Nerve Block….
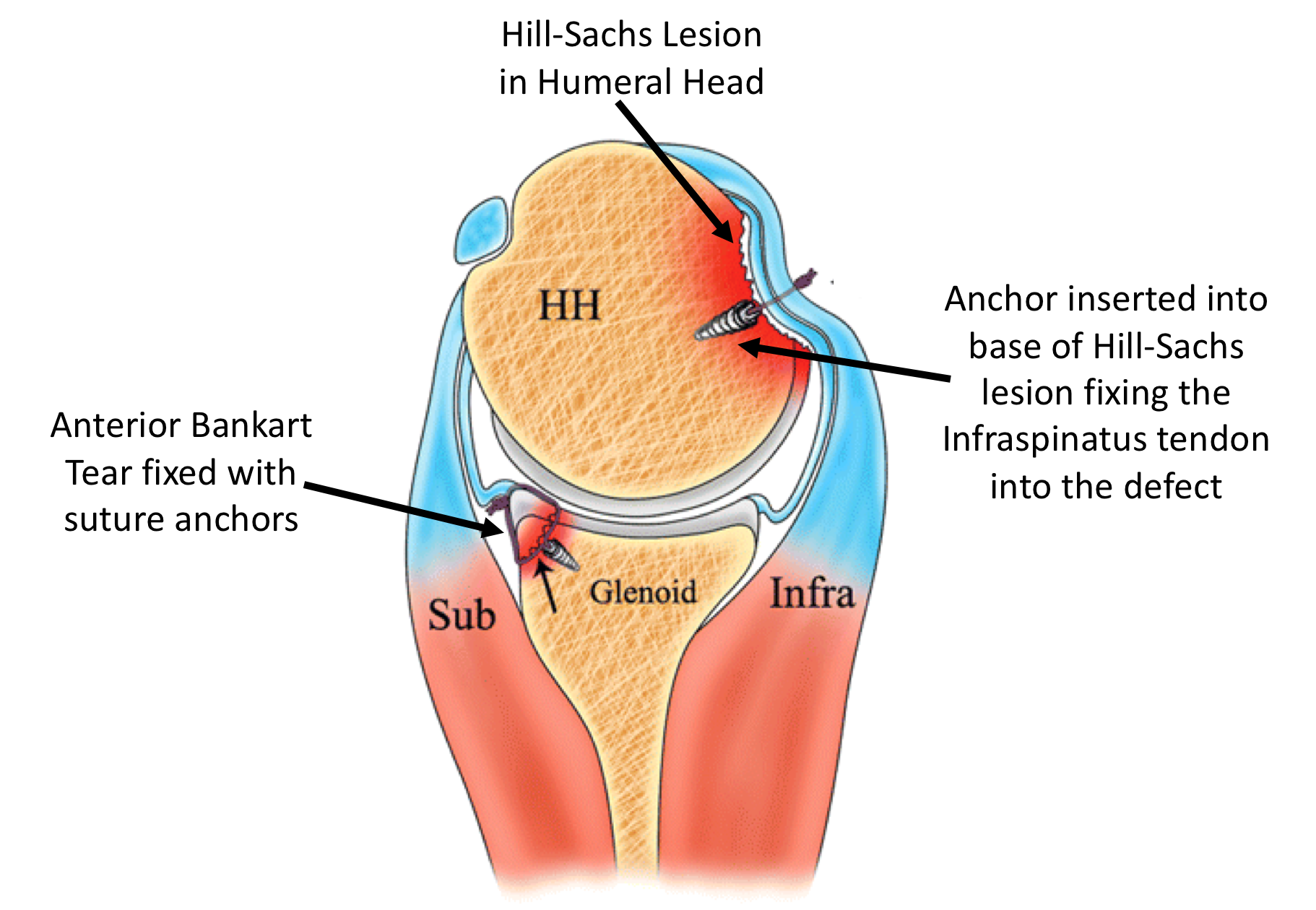
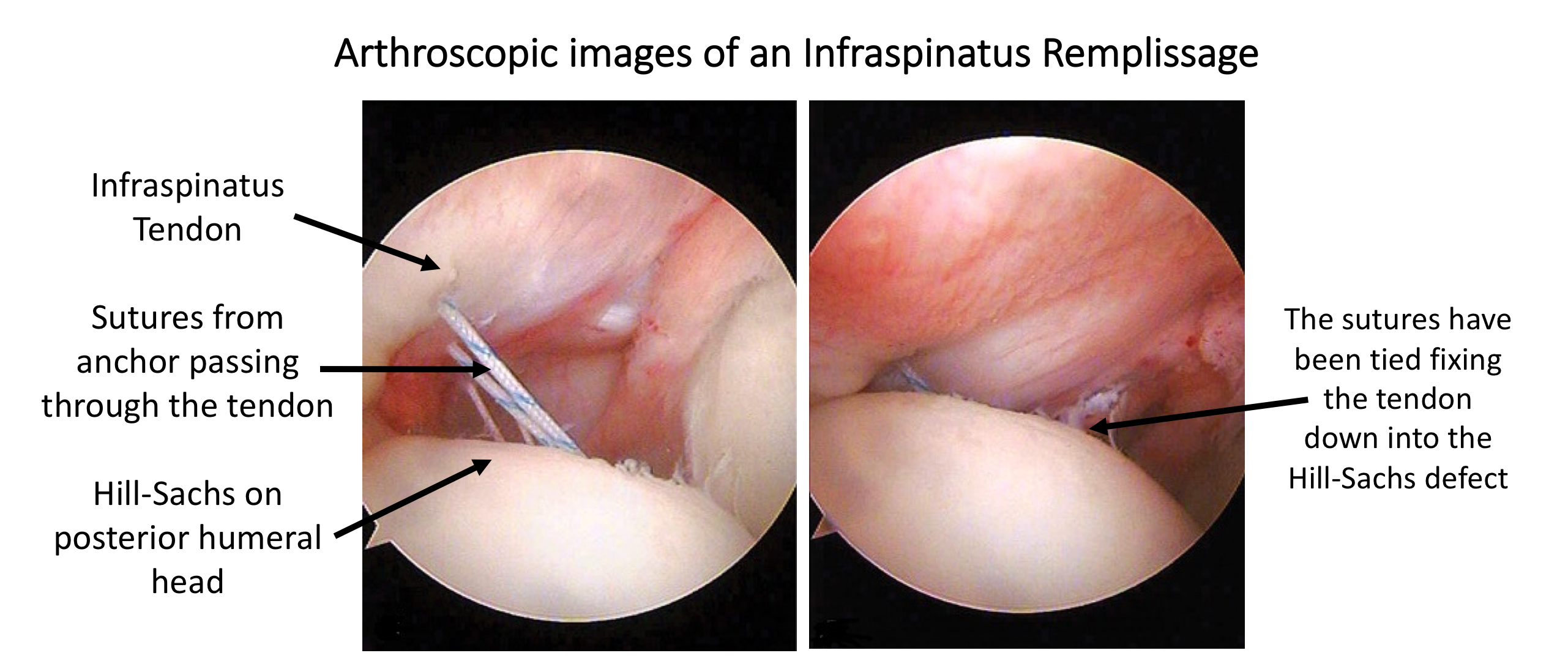
This procedure can be done using an arthroscopic technique, securing the tendon to the bone using suture anchors. The rational is that the tendon will heal into the bone defect so that, when the humeral head rotates into external rotation, the newly fixed tendon will prevent the defect from engaging with the humeral head. Although this initial restricts external rotation, it can recover over time.






I undertake all of my Posterior Stabilisations arthroscopically. There are a number of different variations to the technique and different implants that can be used. I have evolved my technique over the past 15 years, taking advantage of new implants and equipment, and have obtained consistently good results, with which I am happy. My routine Arthroscopic Posterior Stabilisation Procedure is described below,
Watch a video of an arthroscopic Posterior Repair….
Find out more about Arthroscopic Shoulder Surgery….
Procedure
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
- Prophylactic iv antibiotics are given
- A Trimano arm holder is used to hold the patient’s arm in external rotation
- A posterior, 1 - 2 anterior and a Wilmington portal are used for joint access
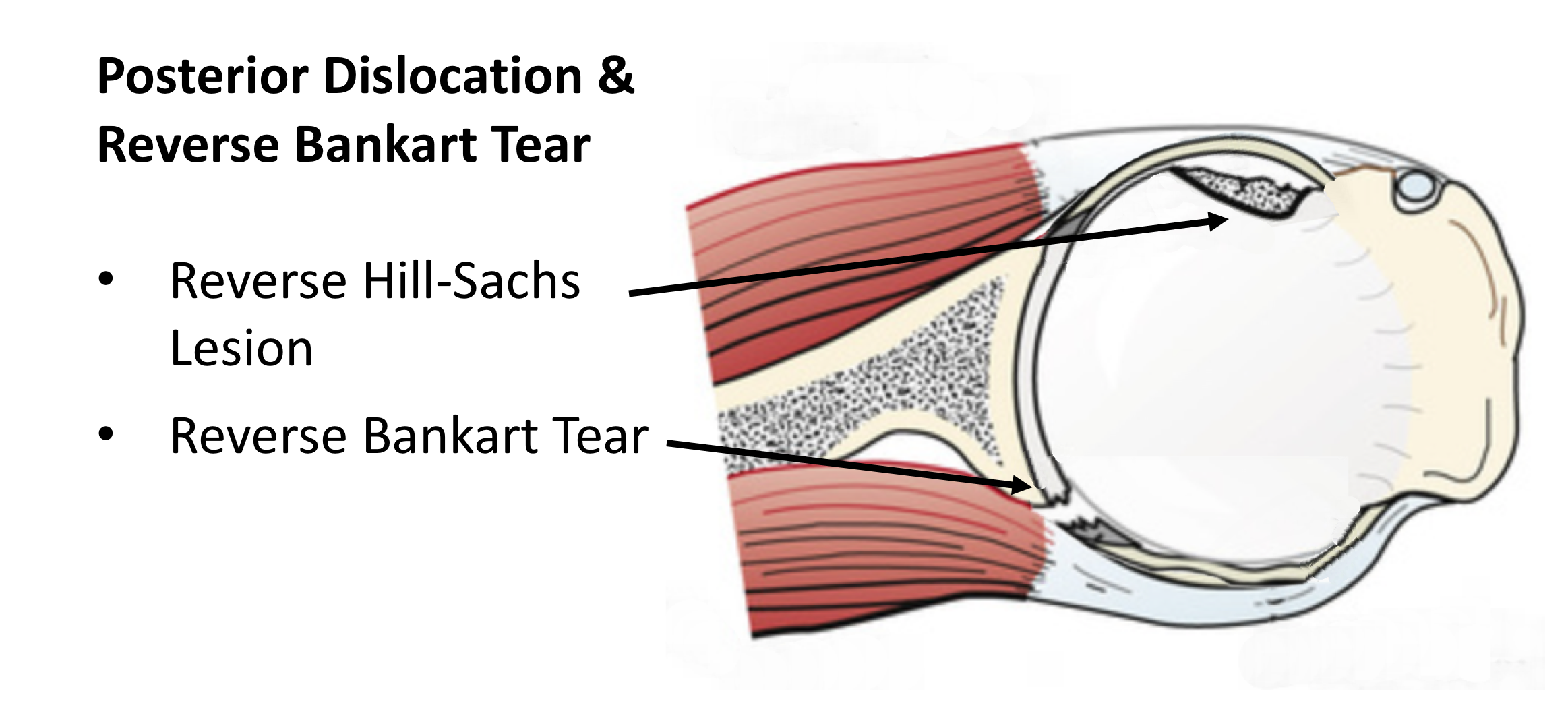
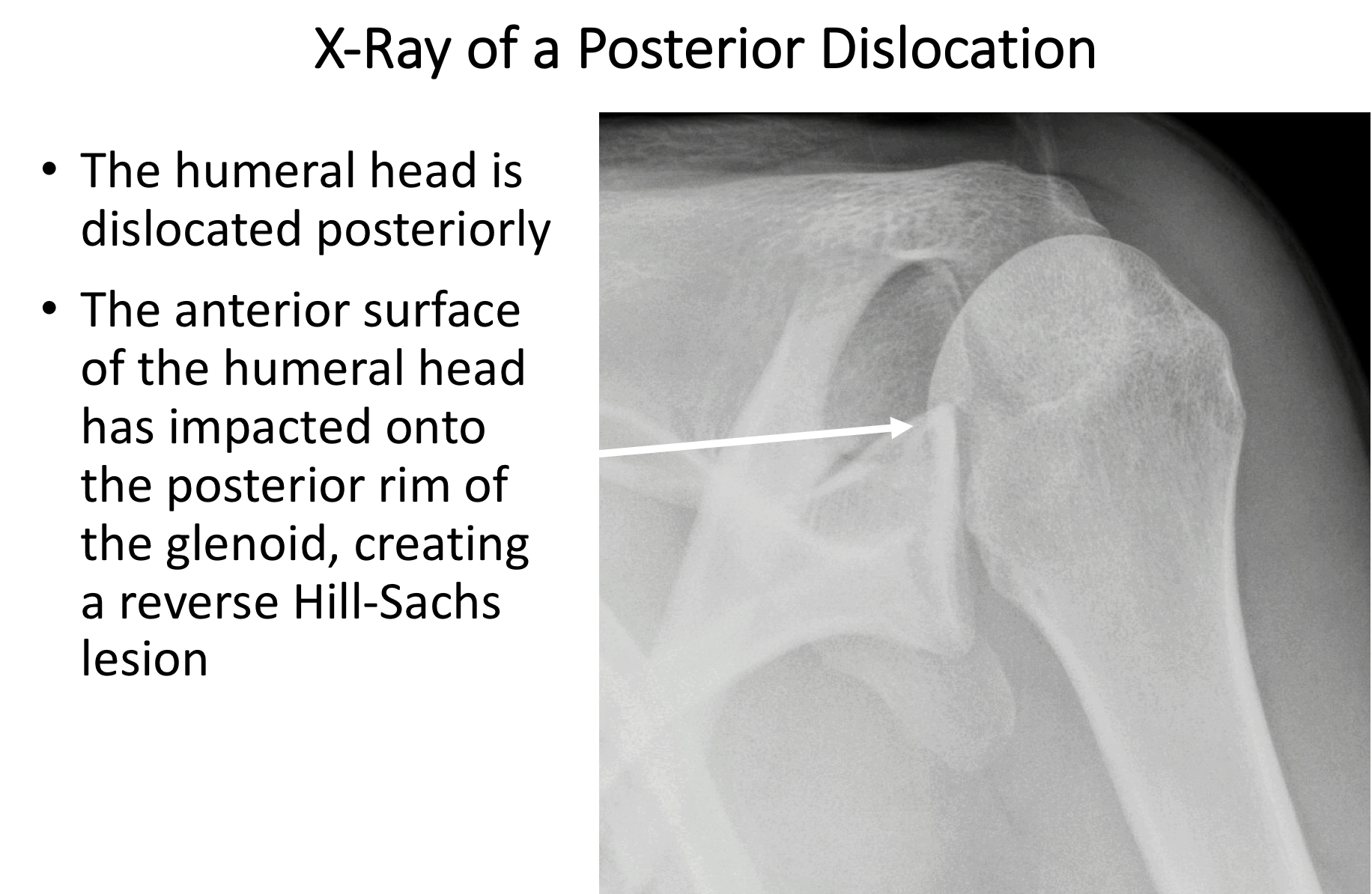
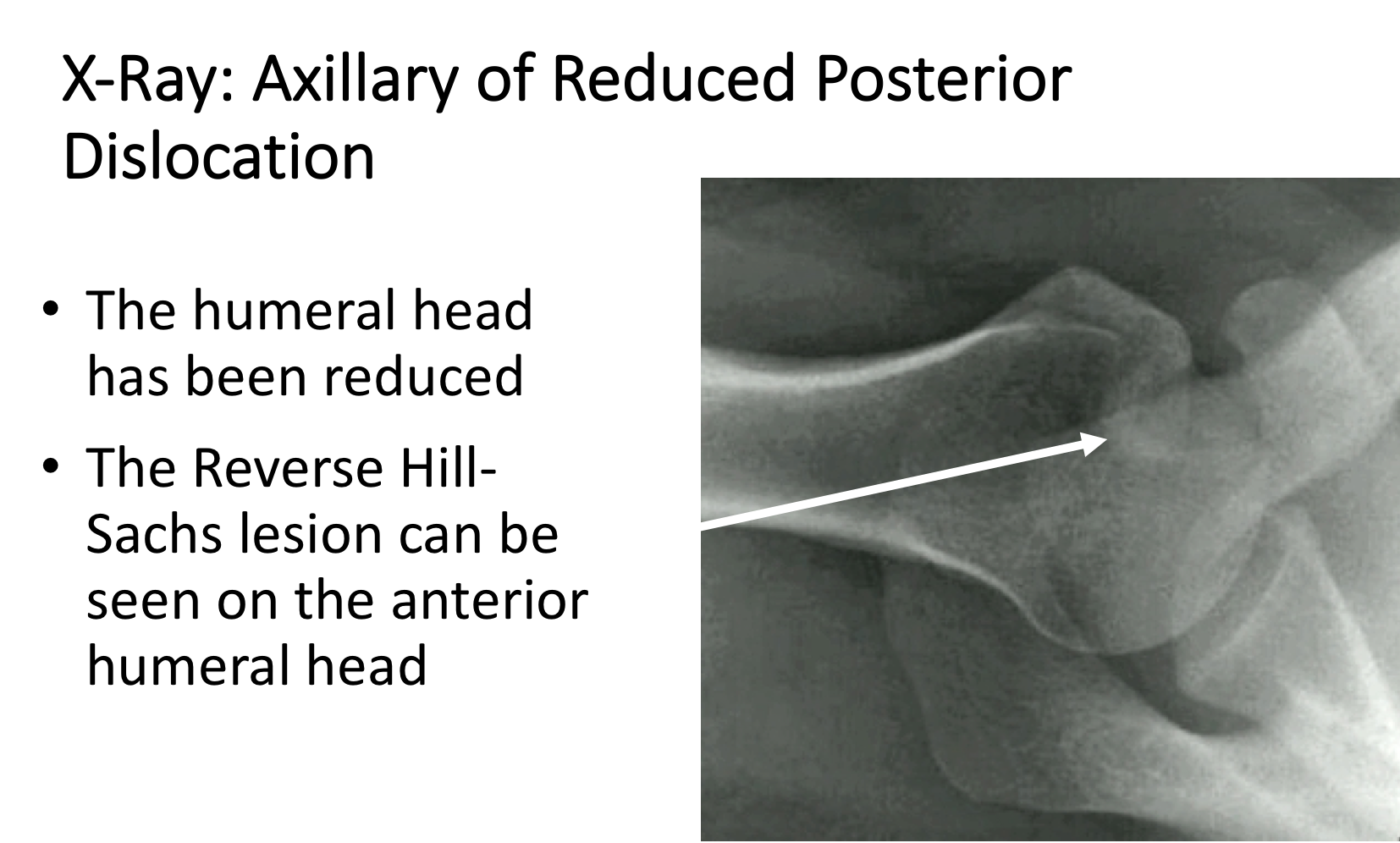
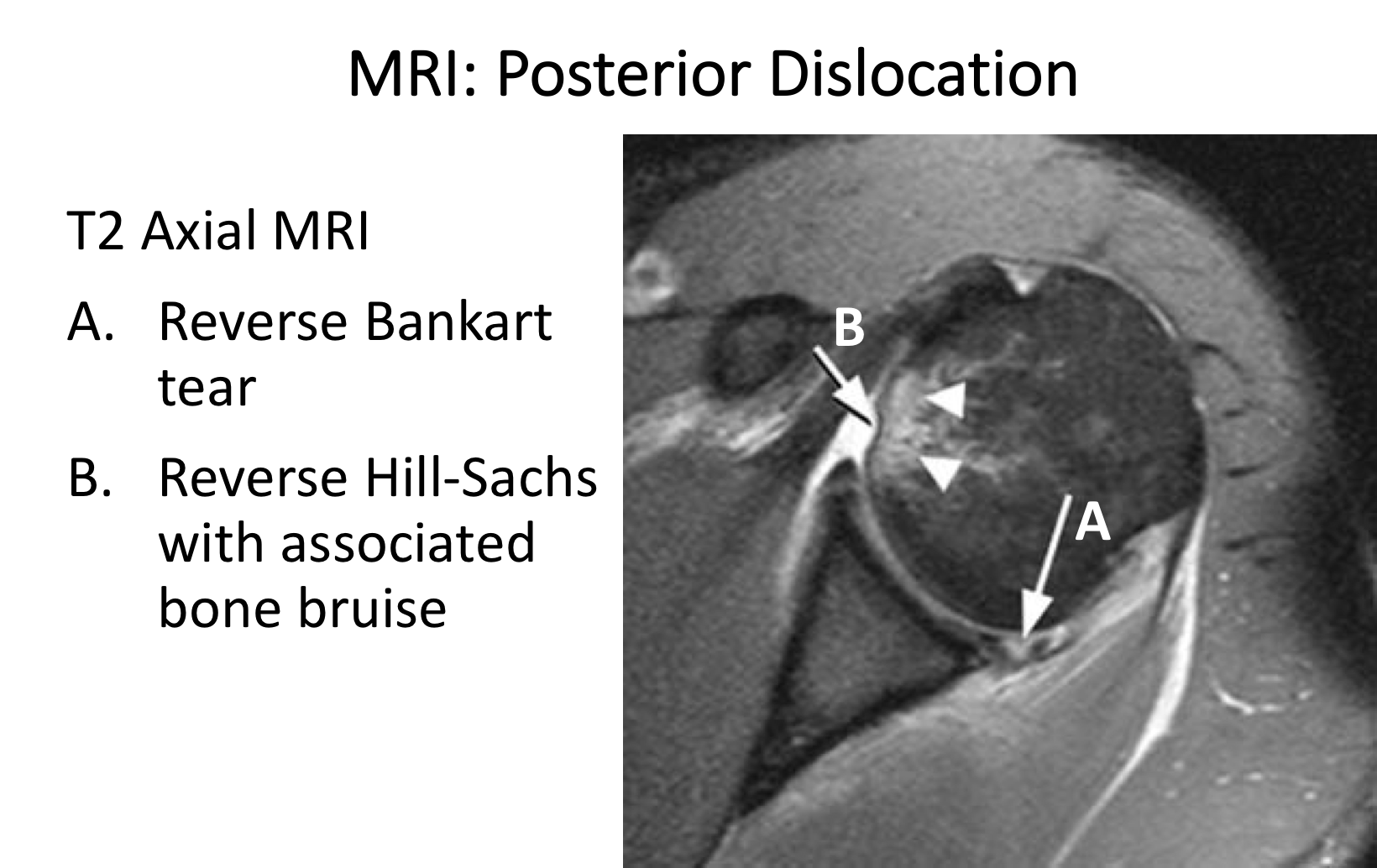
- The joint is initially assessed to confirm the presence of a Posterior Capsular Tear, to assess the extent of any Reverse Hill-Sachs Lesion or Glenoid Bone Loss and any other pathology
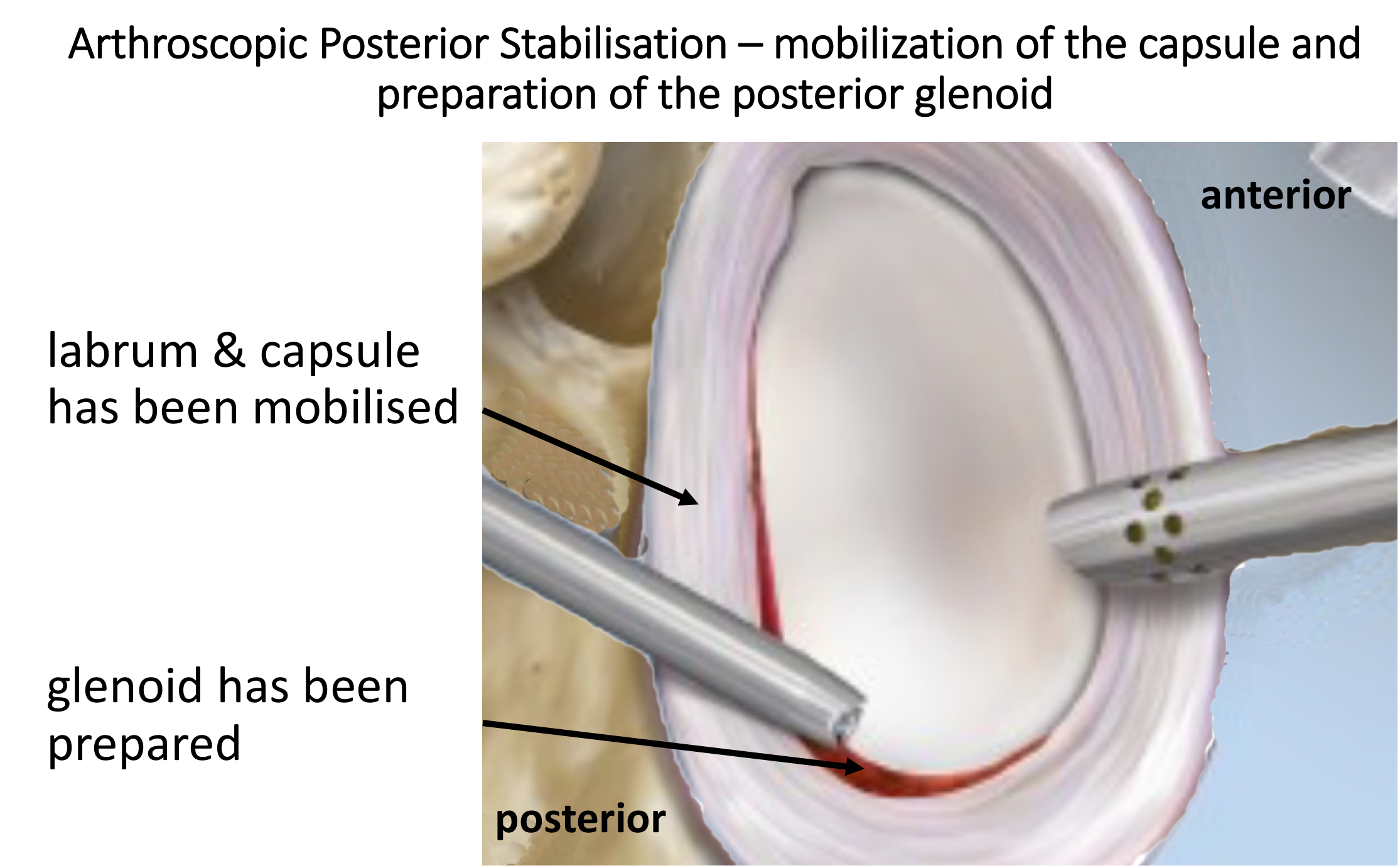
- The Posterior Capsular Tear is then fully mobilised and the tissues freshened
- The Posterior Glenoid is then prepared and freshened
- 3 Osteoraptor or Pushlok bio-composite anchors are inserted into the anterior, inferior glenoid and the capsule and ligaments re-attached with a superior shift
- The repair is assessed and the wounds closed

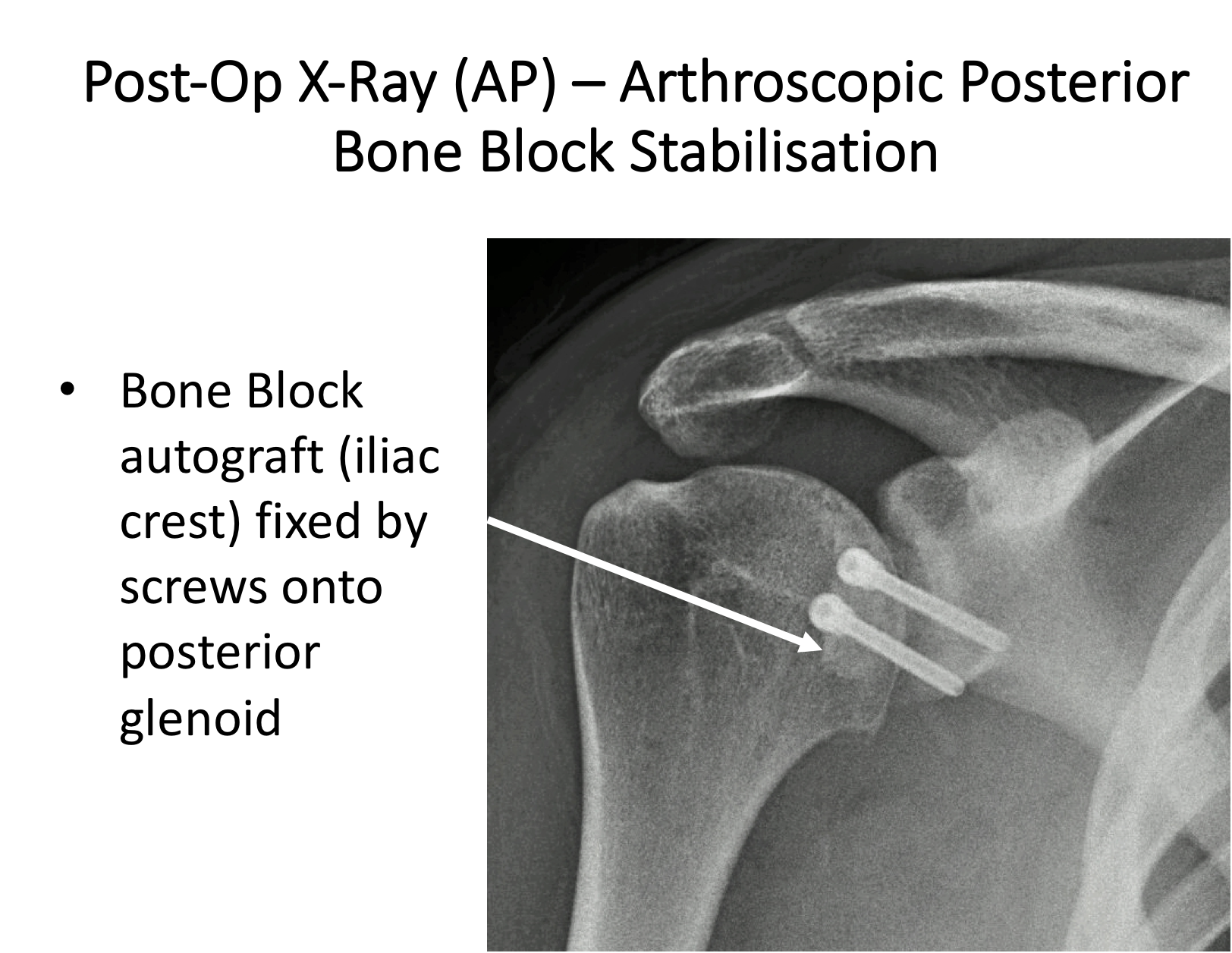
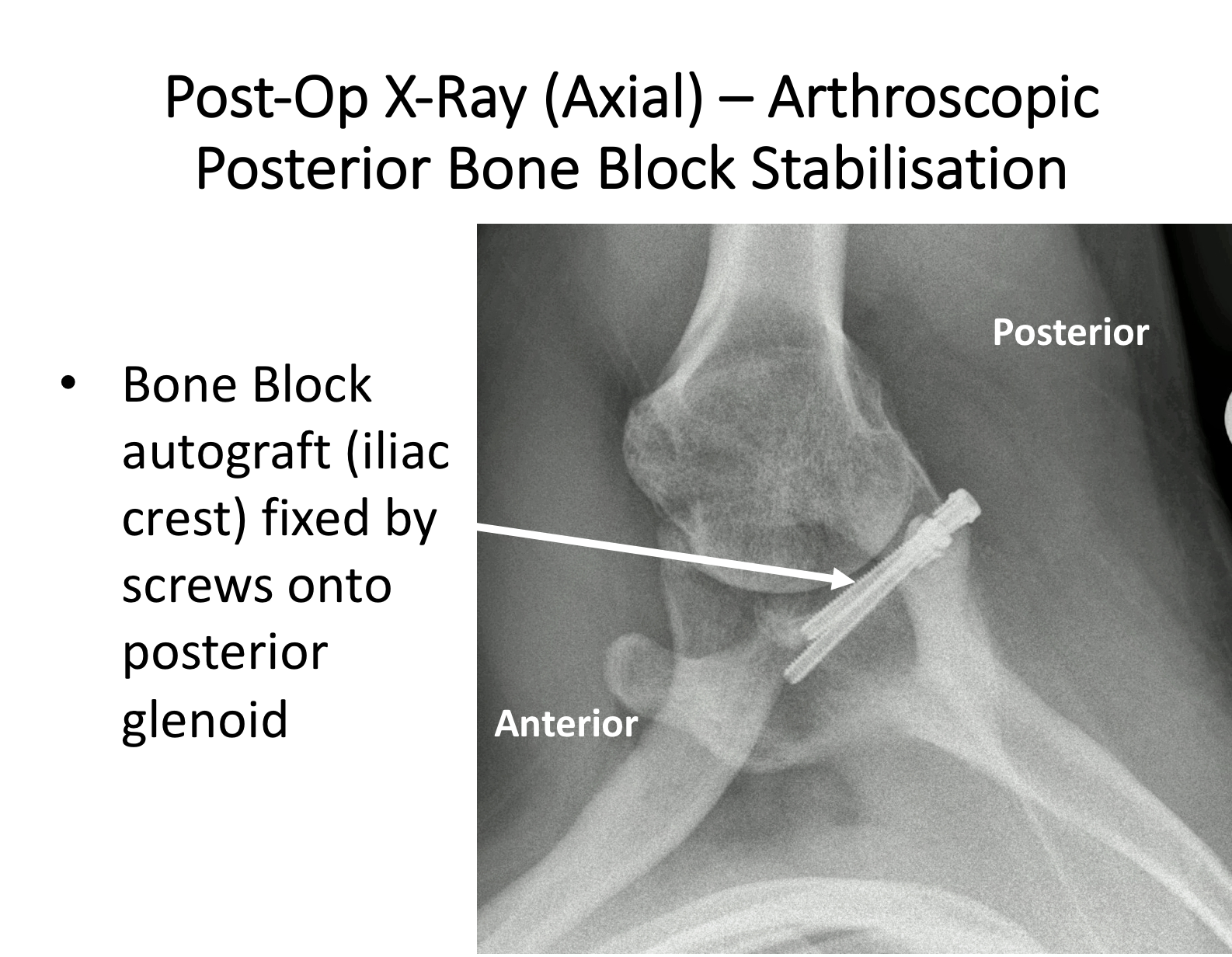
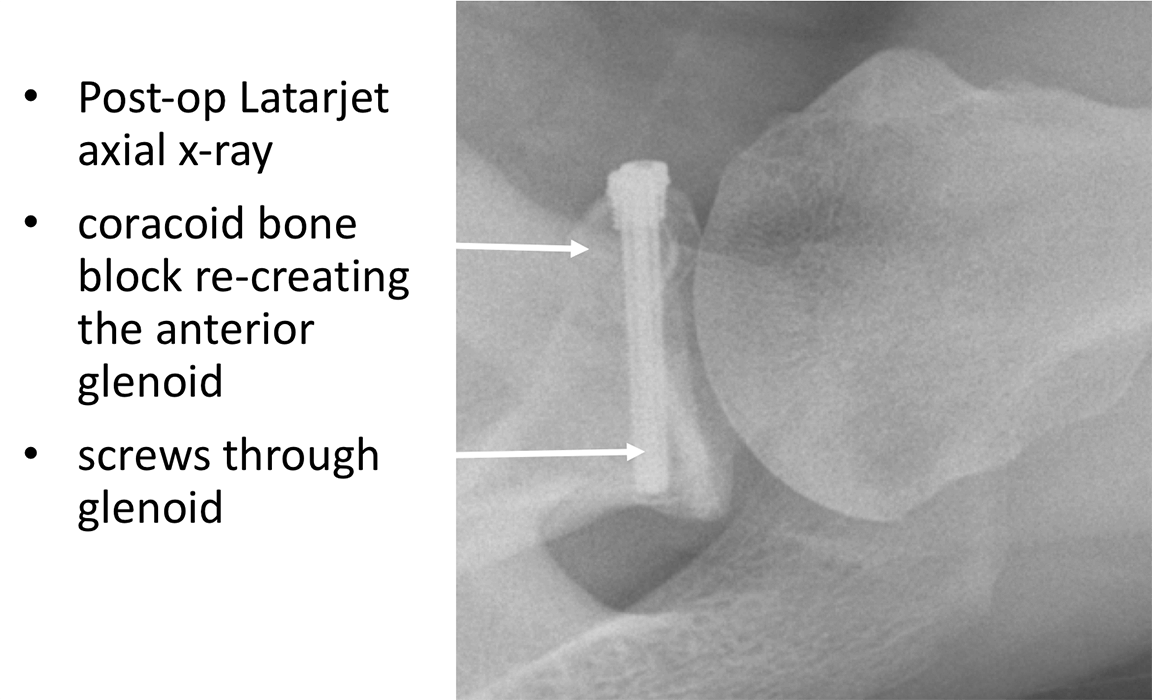
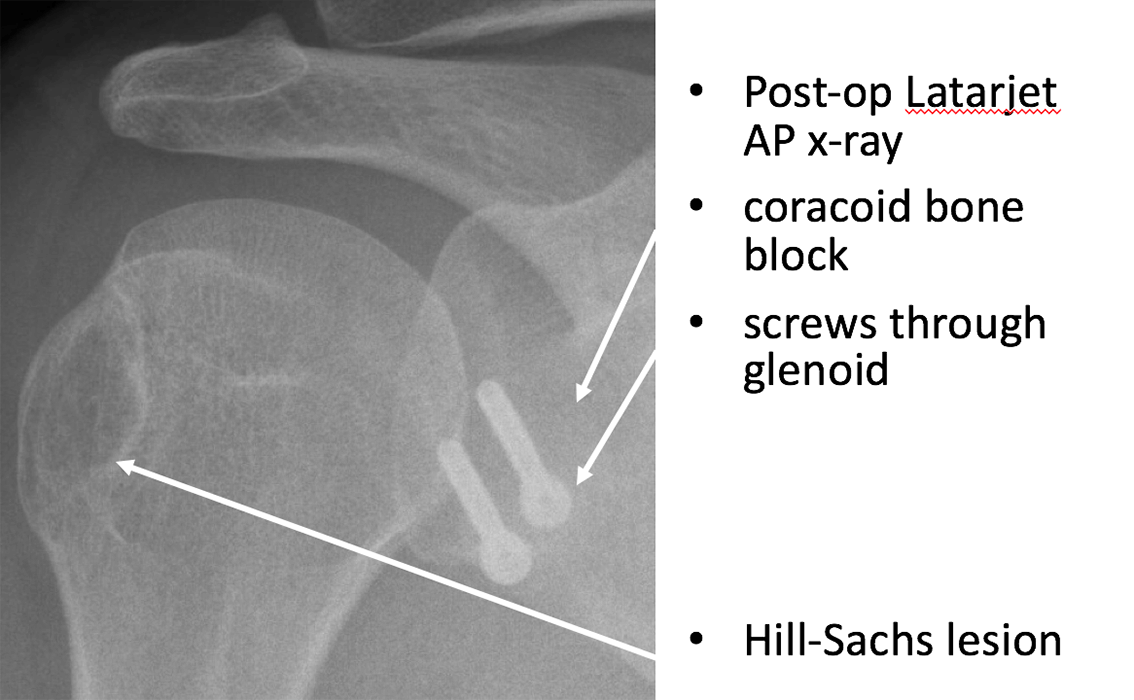
The shoulder is then arthroscoped and the Posterior Glenoid defect prepared. Through a 3 cm longitudinal incision at the back of the shoulder the infraspinatus muscle is split and, under arthroscopic vision the bone block inserted into the joint. Once the bone block is in a satisfactory position, 2 guide-wires are drilled through the guide and bone block into the glenoid. The wires are then over-drilled with a 3 mm drill bit and two 4mm diameter cannulated, partially threaded screws inserted, securely fixing the bone block onto the back of the glenoid. Following this the posterior capsule is then re-attached to the native posterior glenoid using suture anchors. This exteriorises the bone block, protecting the humeral articular surface.

Watch a video of an arthroscopic Posterior Bone Block Procedure….
Find out more about Arthroscopic Shoulder Surgery….