SLAP / Labral Tears
What is a SLAP/Labral Tear?
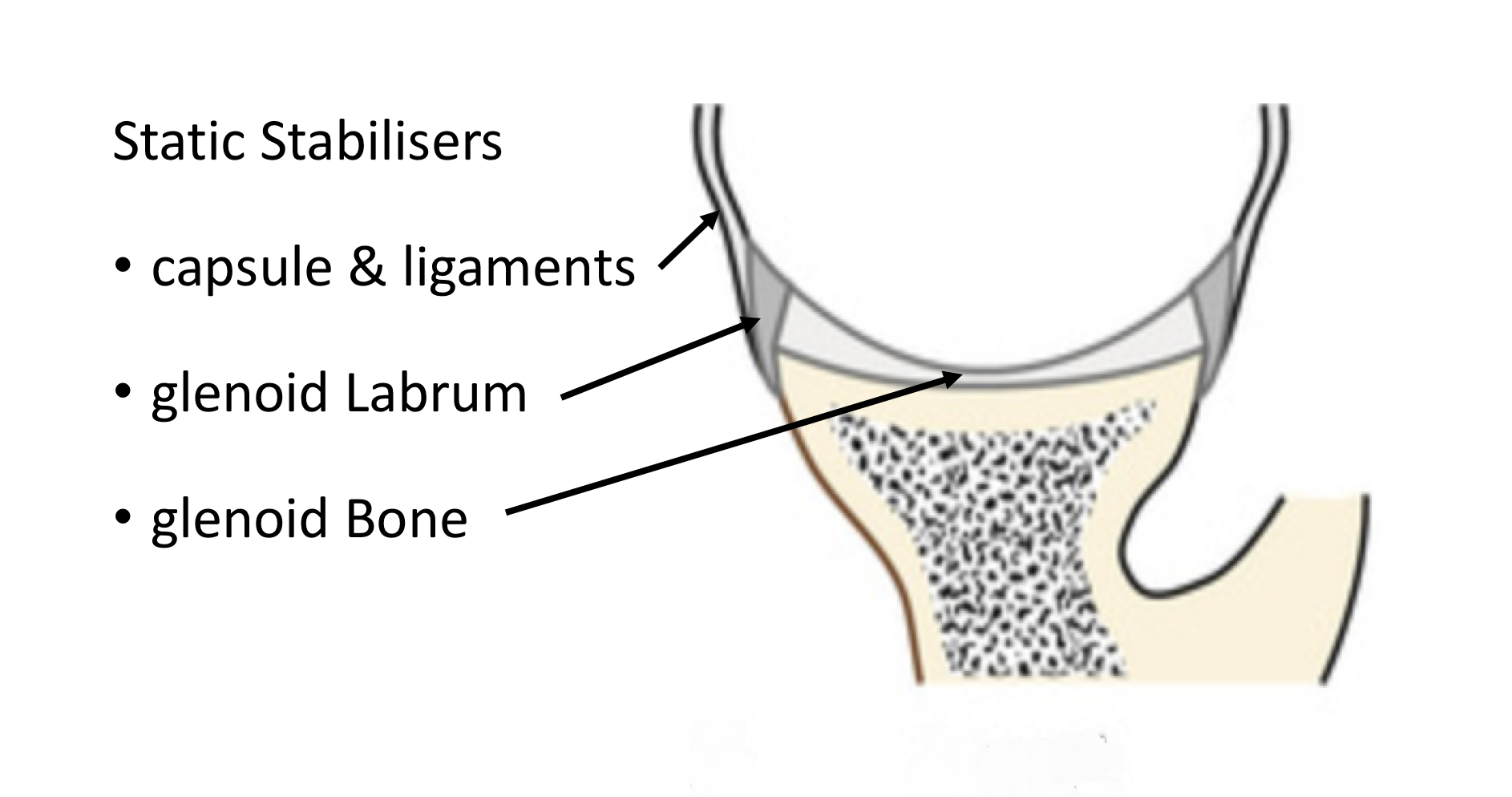
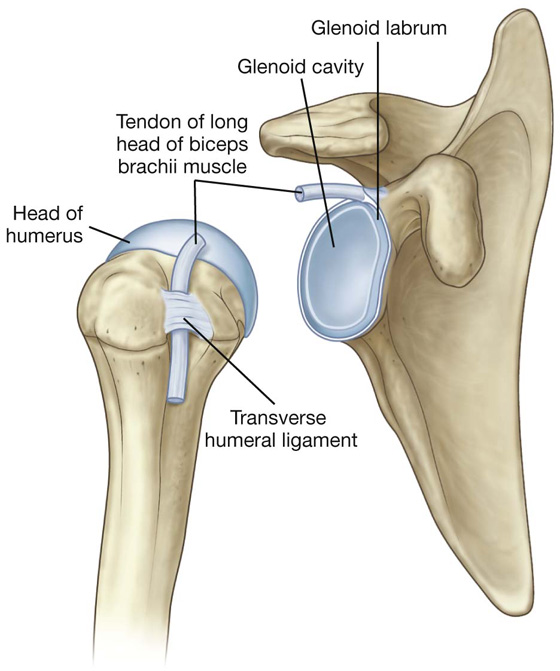
The shoulder has a large ball (humeral head) and a relatively shallow socket (glenoid). This allows for a large range of movement but, potentially, is very unstable. The shoulder rarely dislocates because it is stabilised by a number of soft-tissue structures that surround it. The Glenoid Labrum is one of the stabilising soft-tissue structures that surround the shoulder.
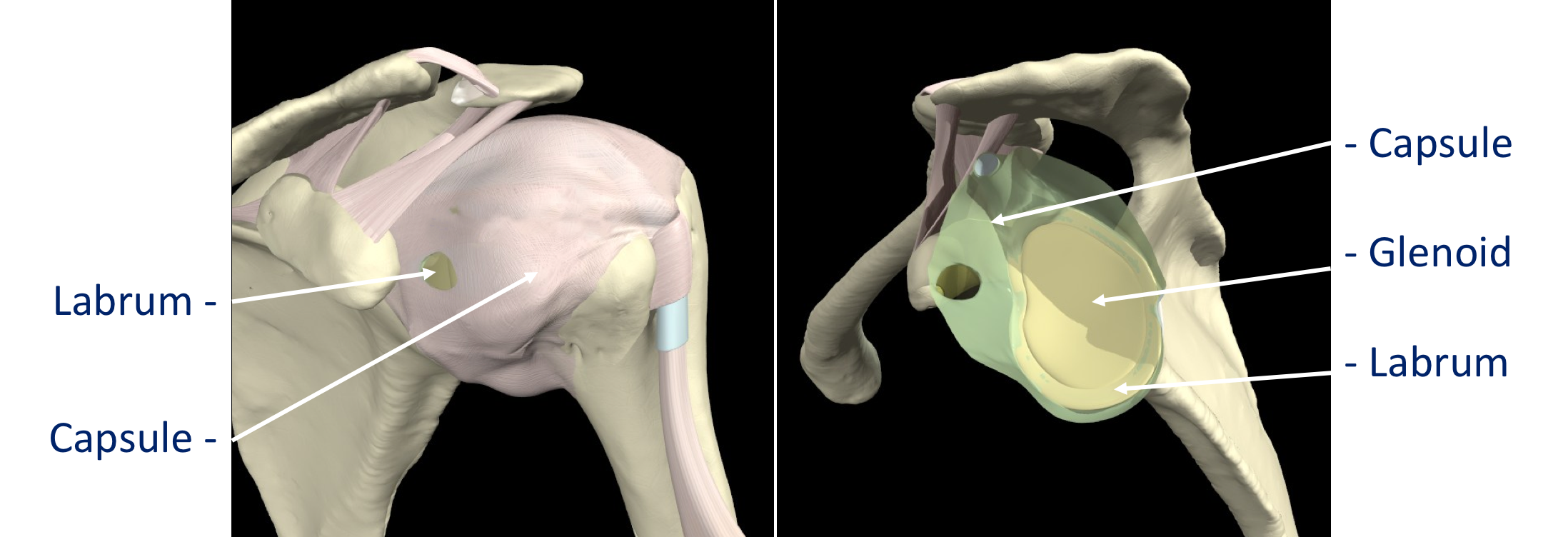
The Glenoid Labrum is a rim of fibrous tissue that surrounds and deepens the glenoid socket, increasing stability. Mechanically it doubles the effective concavity/depth of the socket.
Find out more about the stabilising structures and the anatomy of the shoulder….

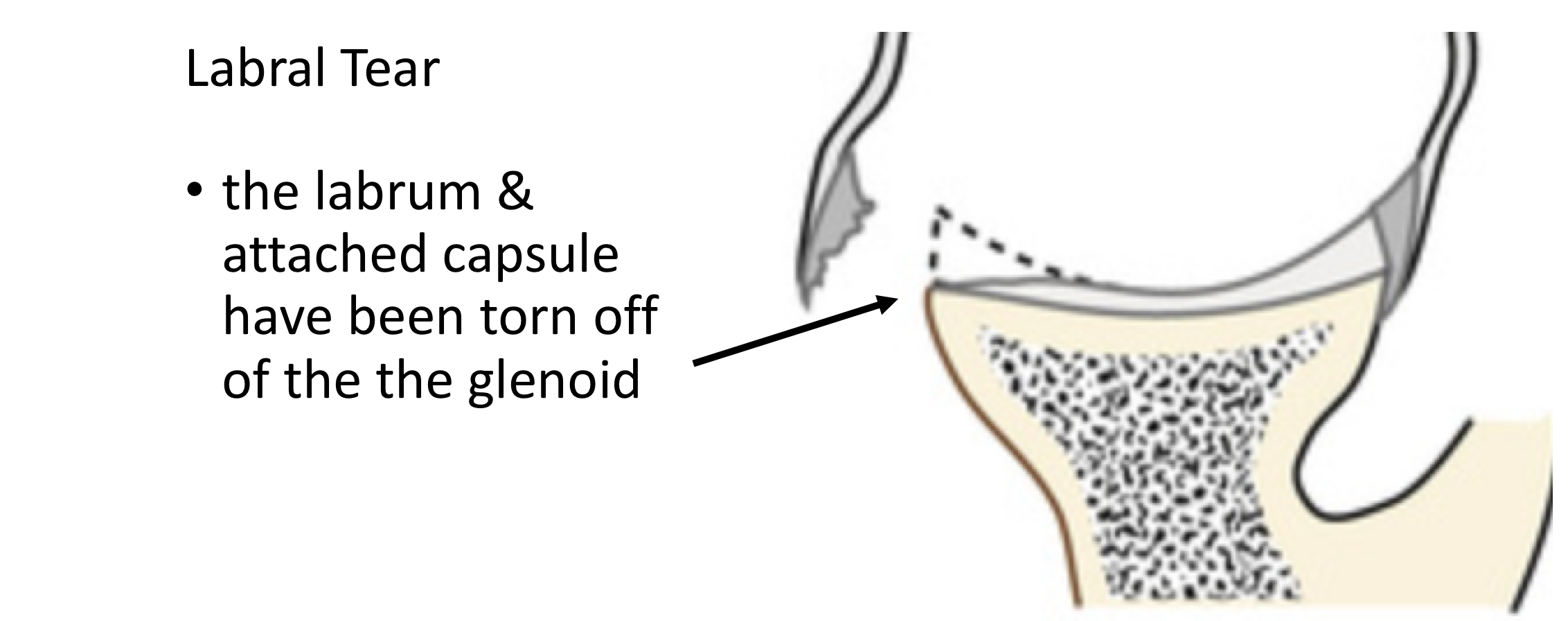
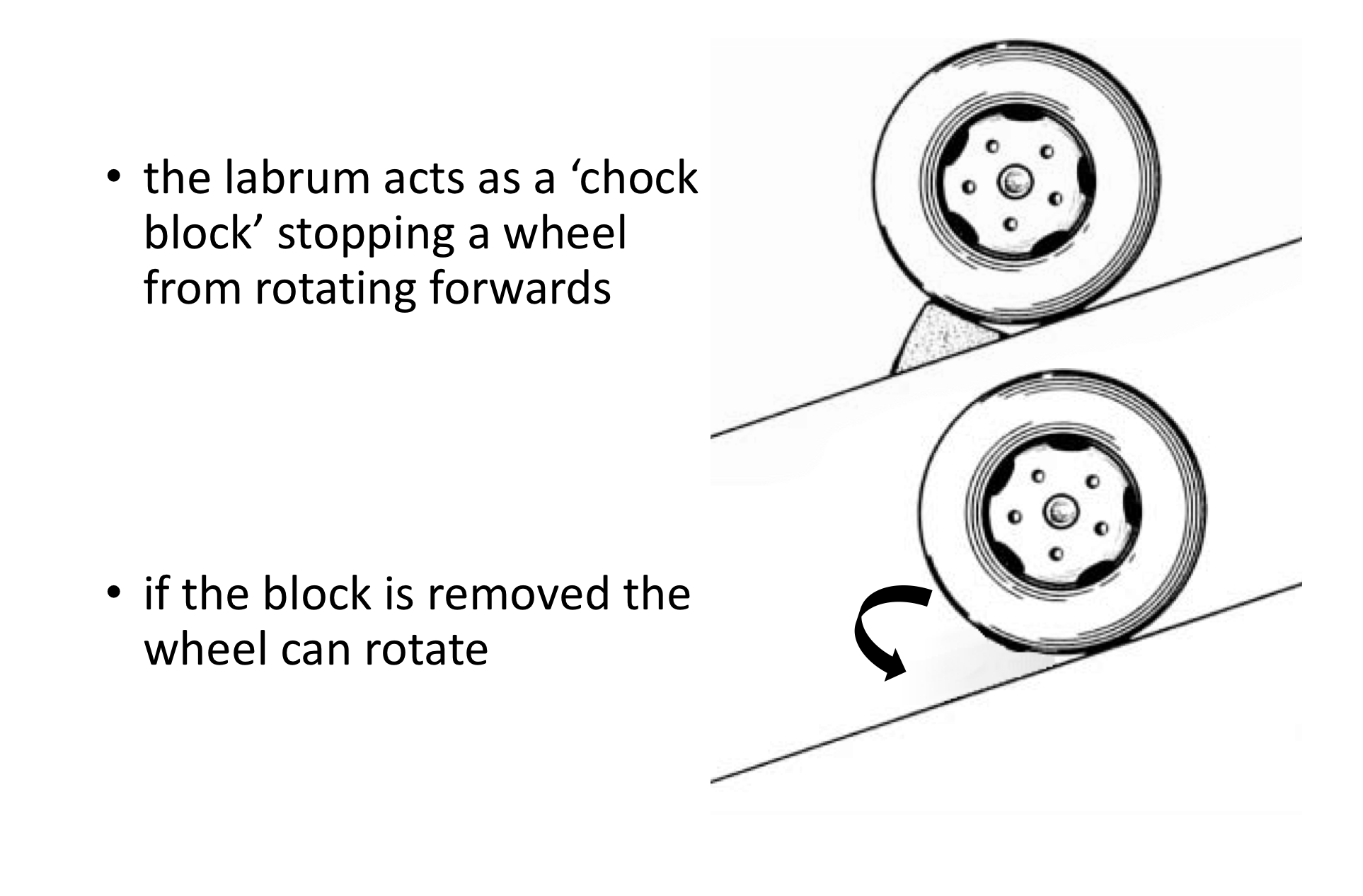
If the Glenoid Labrum is damaged, and torn away from its attachment to the glenoid socket, the stability of the shoulder can be affected. Whilst the Glenoid Labrum is not a major stabilising structure of the shoulder, problems associated with a Labral tear tend to be with micro-instability, a feeling that the shoulder is slipping or issues with throwing, rather than the shoulder completely dislocating. The labrum can be likened to a ‘chock block’ that stops a wheel from rotating forwards, when it is damaged the humeral head can slip forwards.
The labrum can be likened to a ‘chock block’ that stops a wheel from rotating forwards, when it is damaged the humeral head can slip forwards.
A SLAP Tear is a specific type of labral tear in a specific position on the Glenoid. It stands for a Superior Labral Anterior to Posterior Tear.
The Long Head of Biceps tendon inserts into the superior part of the Glenoid Labrum. Damage to the Labrum, where the Long Head of Biceps attaches, can cause problems with the Long Head of Biceps, and, conversely, the Long Head of Biceps can cause traction injuries to the Glenoid Labrum.
Find out more about the Long Head of Biceps….
Types of SLAP Tears
All SLAP tears involve damage to the Glenoid Labrum where it attaches to the superior part of the Glenoid socket. Different types of injuries can occur and these have been classified into various types. Although more than 12 types of different tears have been described only Types 1 to 5are really of clinical significance.
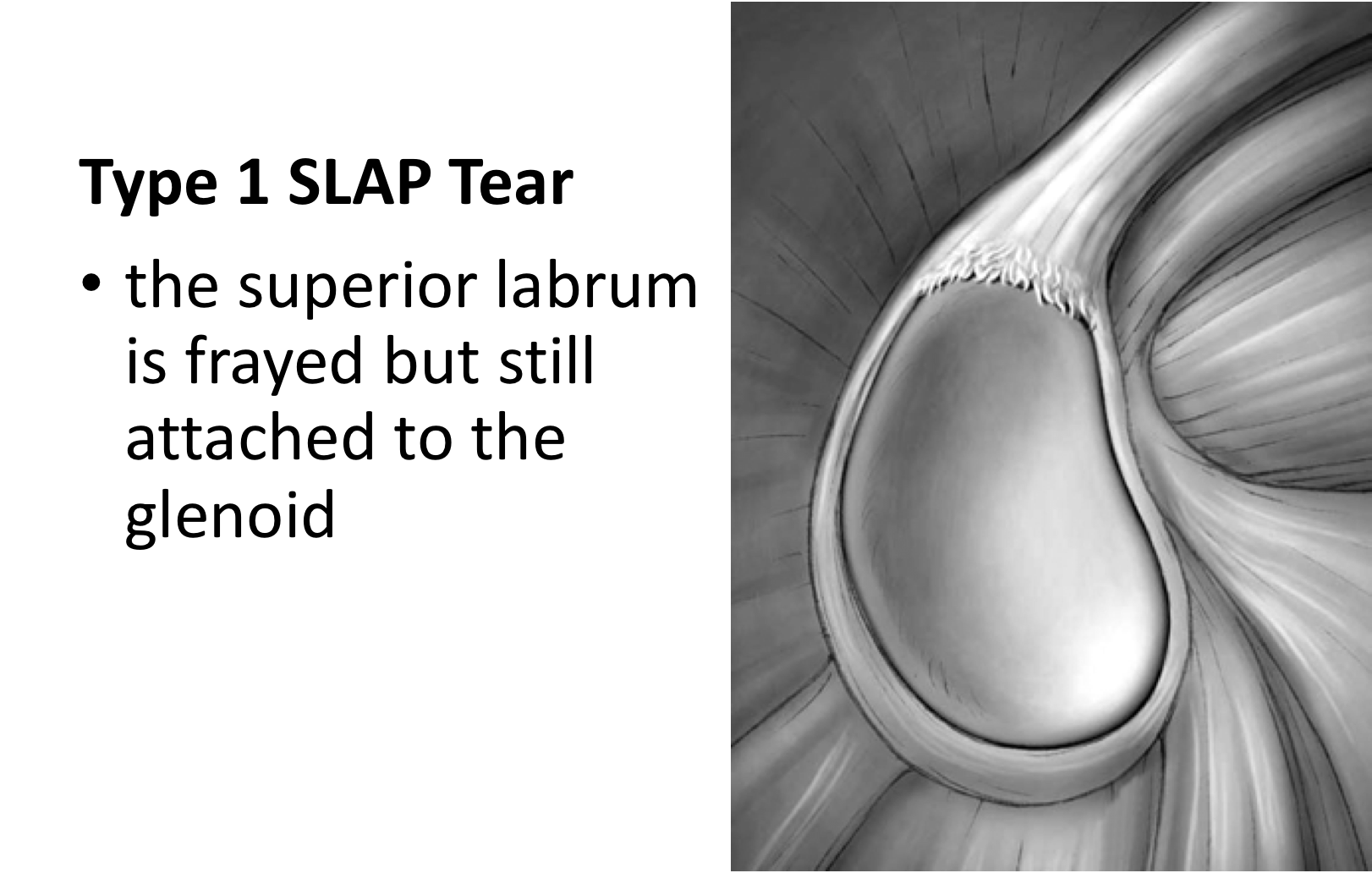
Type 1 SLAP - This is the most minor type of tear and represents tearing and fraying of the Labrum where it attaches to the superior Glenoid. The labrum is still attached to the glenoid.
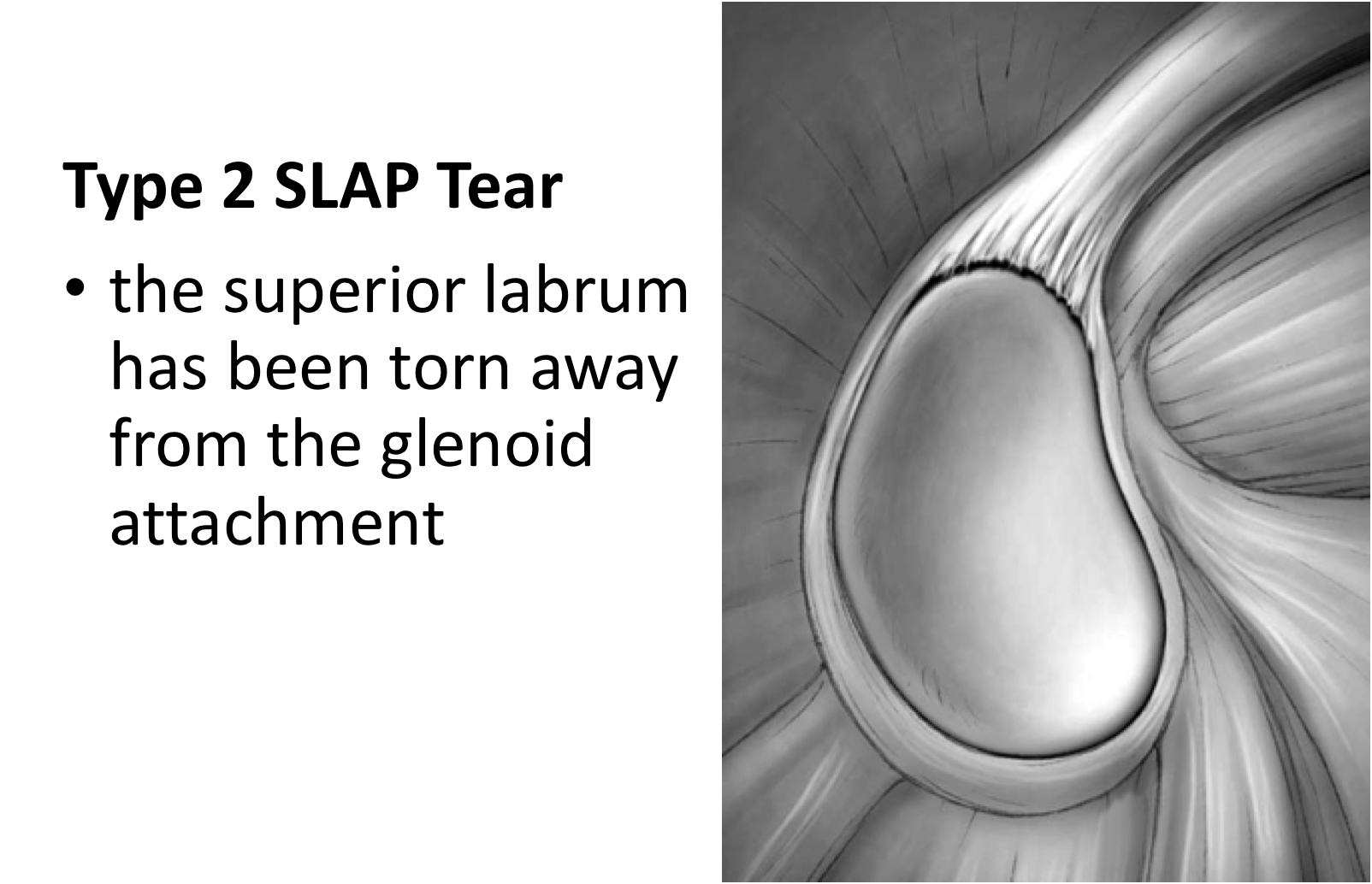
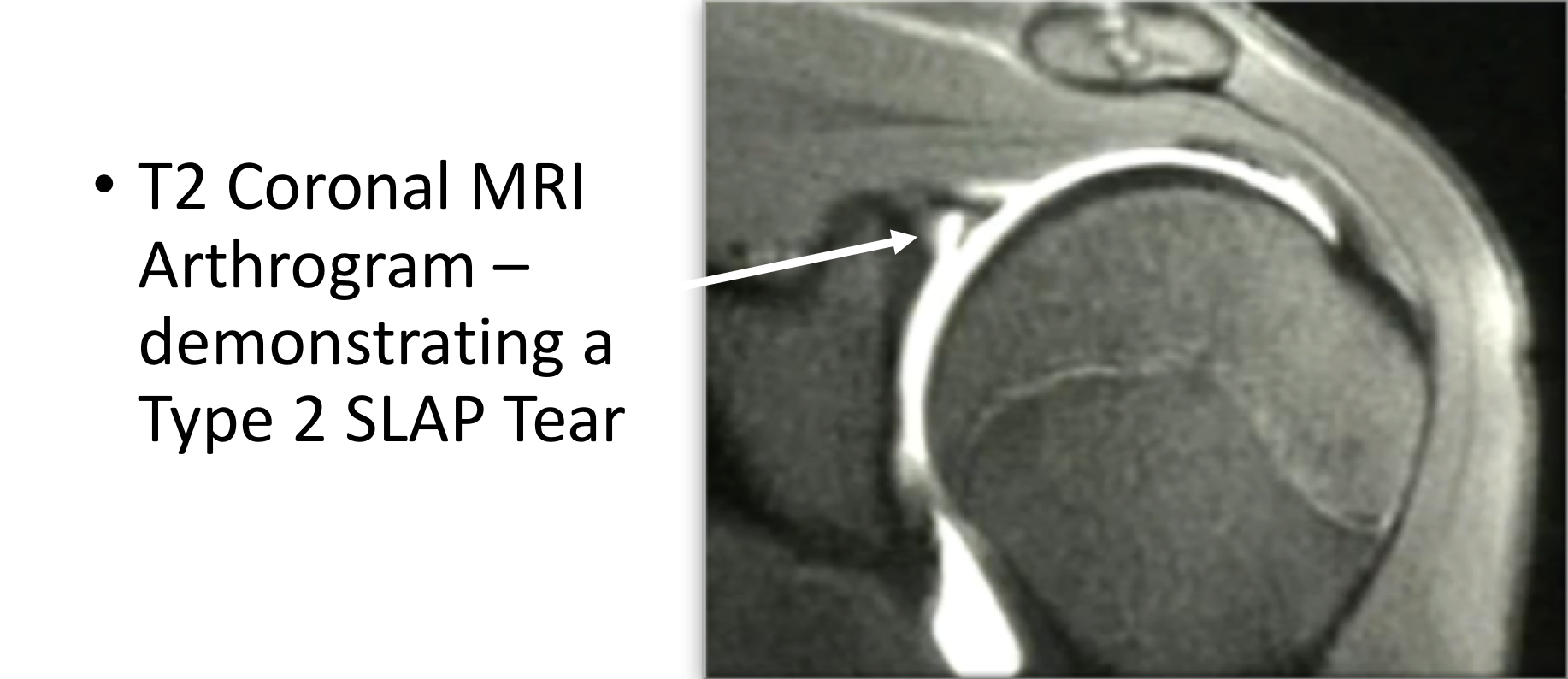
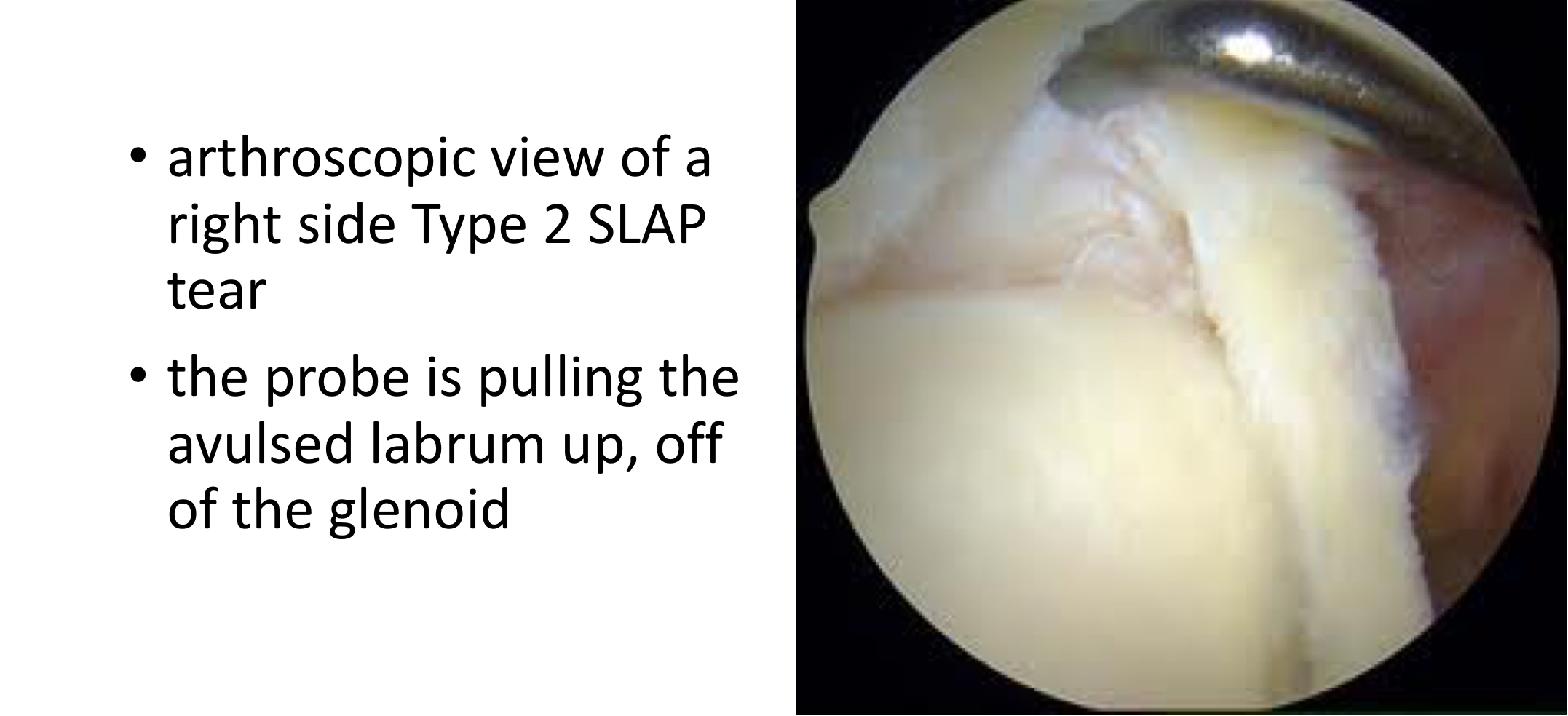
Type 2 SLAP - This represents tearing of the labrum off of the superior glenoid. In this type of tear the Long Head of Biceps attachment to the glenoid has been damaged.
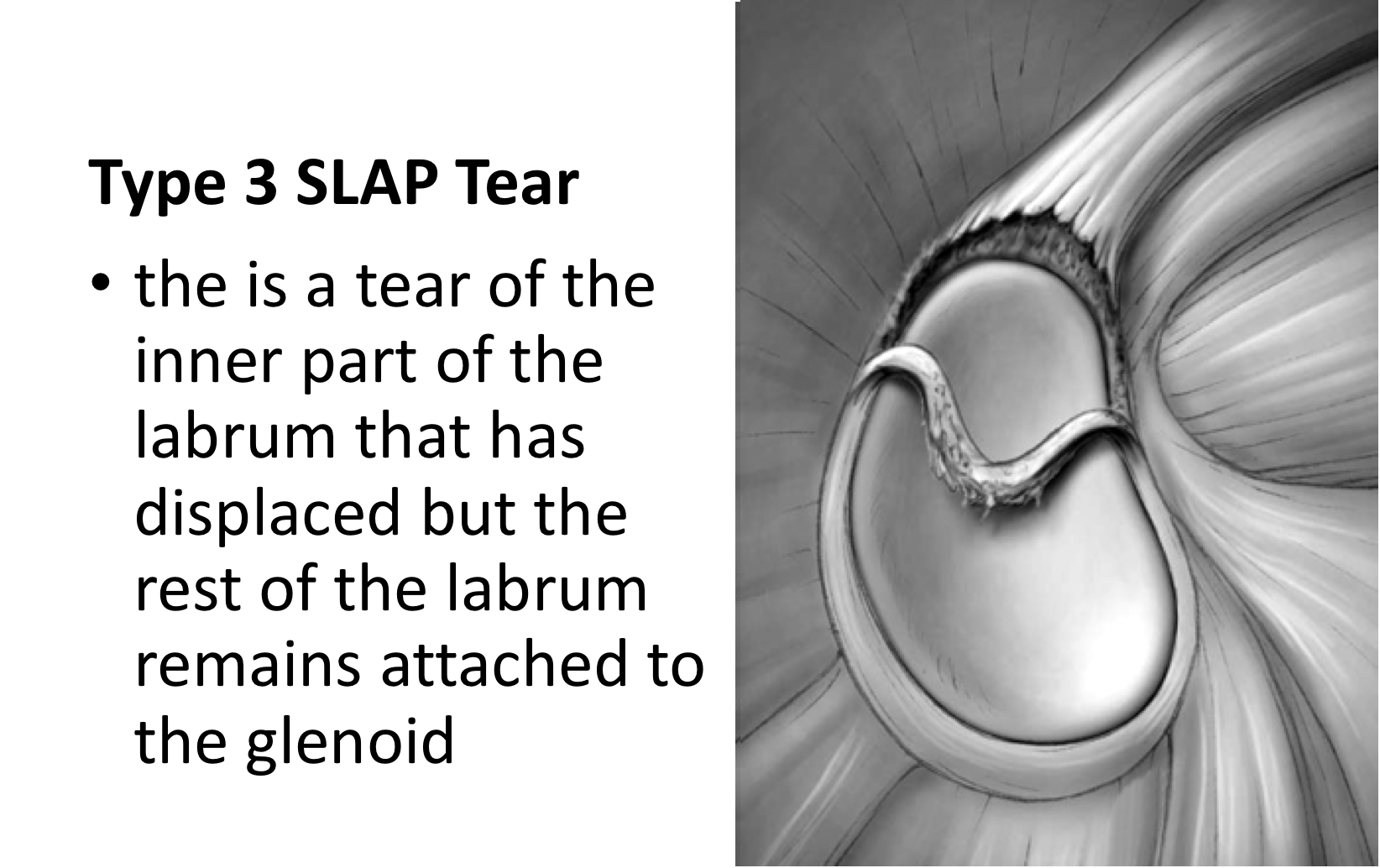
Type 3 SLAP - This represents a tear and split of the inner half of the labrum. The torn bit of labrum will usually ‘flop down’ into the joint. The outer part of the labrum is still attached.
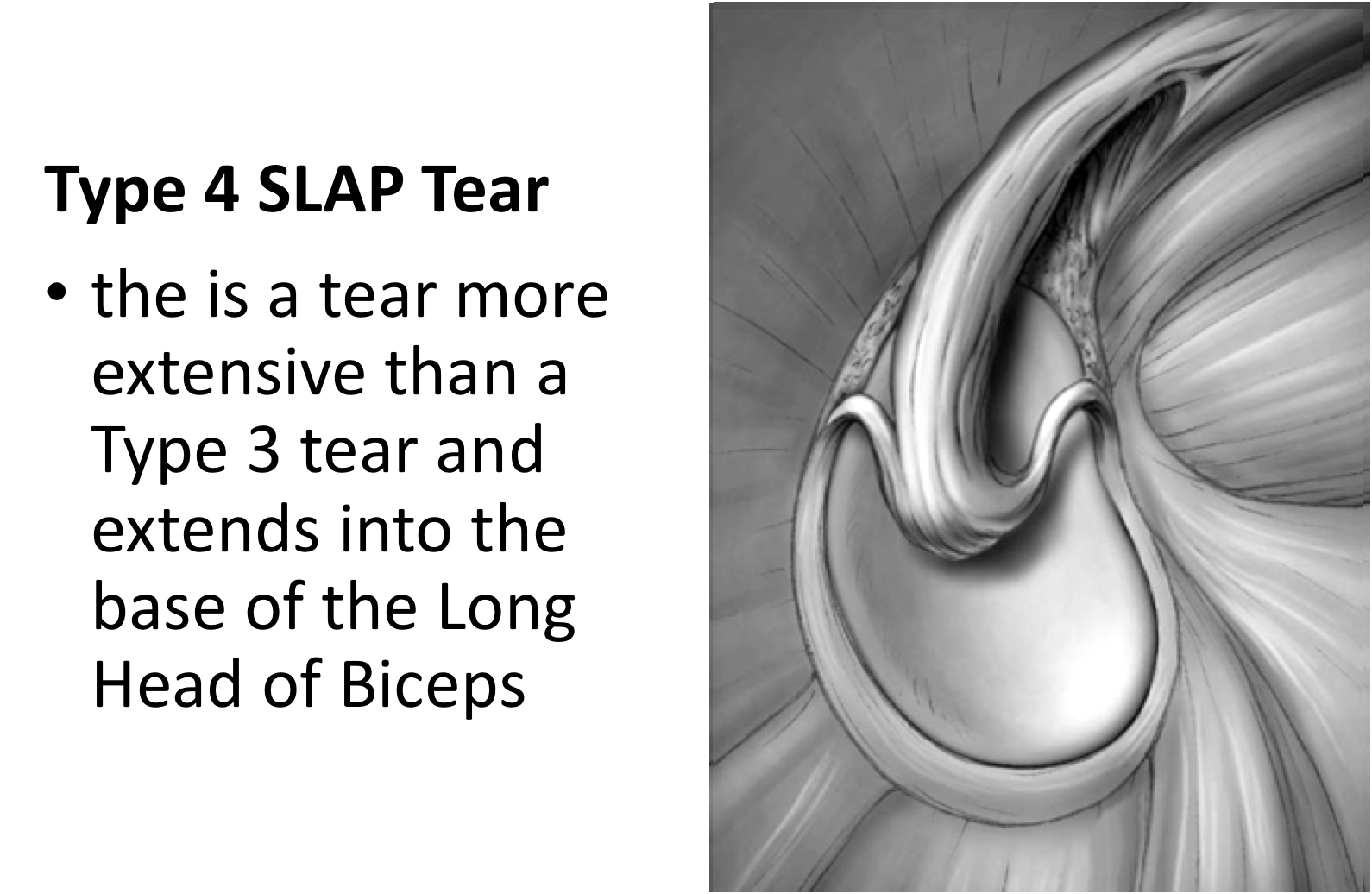
Type 4 SLAP - This is a more severe version of a Type 3 tear in which the split passes into the Long Head of Biceps. This type of tear may cause problems with the Biceps tendon.
Type 5 SLAP - This is a more extreme version of a Type 2 SLAP tear where the tear has continued down the front of the glenoid to become an additional Bankart tear. These types of tears usually result from a dislocation of the shoulder.
Find out more about Bankart Tears and Shoulder Dislocations….

What Causes a SLAP Tear?
Action of Throwing -
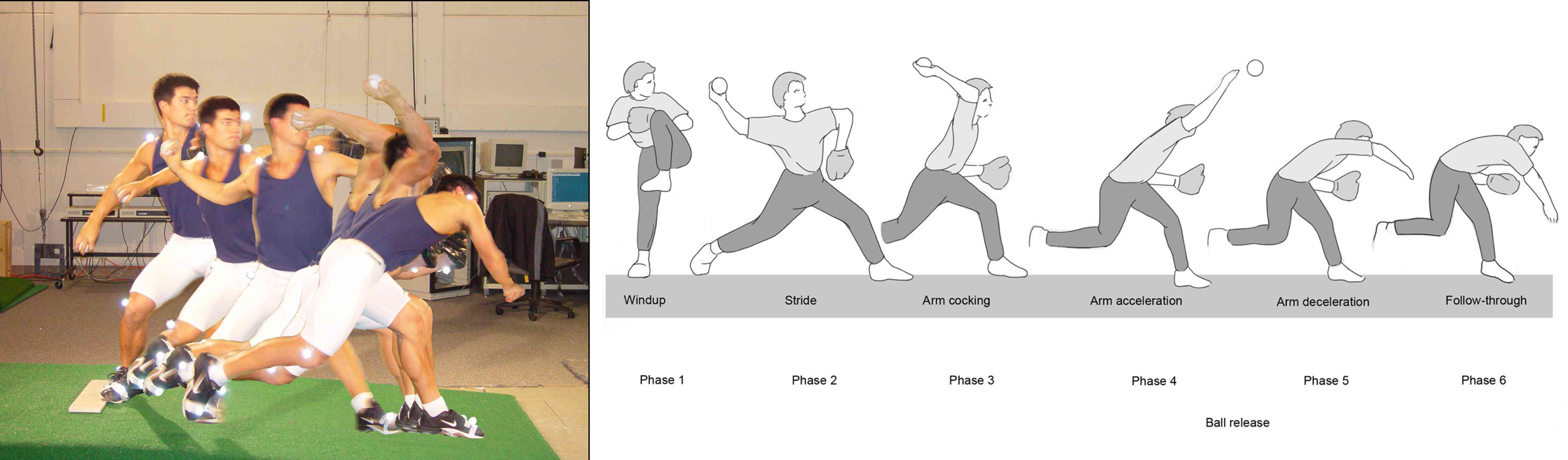
- Throwing is a very complex action and involves generating a massive amount of force & energy from the legs upwards and focusing it through the shoulder to project the arm forward and throw a ball. The action of throwing has been studied extensively and has been divided into 5 phases.
- The Early Cocking and Late Cocking phases ‘store up’ all of the energy. The Acceleration phase releases this energy and ‘fires’ the ball forward. The Deceleration phase involves all of the muscles, ligaments and tendons around the shoulder rapidly contracting to stop the arm. The Follow Through phase allows the weight of the body to drop forwards, helping to dissipate energy.
- SLAP tears can be caused by a single one off injury (Acute) or can be the result of a repetitive action (Chronic) The most common cause of SLAP tears occurs from overhead shoulder activities such as throwing and serving.
Acute SLAP Tears -
- Acute tears tend to occur during the Deceleration phase of throwing or serving. The patient feels an acute pain in their shoulder, sometimes passing down into their biceps and passing backwards.
- Acute tears can also occur as part of a ‘shearing’ injury as the shoulder dislocates anteriorly. Sometimes the shoulder ‘subluxes’ (does not fully dislocate). This can sometimes result in the labrum being ‘knocked off’ creating a labral/SLAP tear.
Chronic SLAP Tears -
- Sometimes the repeated throwing/serving action can lead to a ‘wear and tear’ or overload injury. Over time a SLAP Tear can develop or occur as an Acute on Chronic injury.
What are the Symptoms of a SLAP Tear?
- SLAP / labral tears tend to cause problems related to shoulder stability when doing more ‘complex’ movements such as throwing or exercising. Between episodes of activity patients shoulders . Patients tend to experience pain at the top of the shoulder, which can often be mistaken for an AC joint problem. Pain sometimes passes into the back of the shoulder and also down the arm, into the biceps.
- Patients may notice a feeling of ‘slipping’ or ‘looseness’ in their shoulder. There may also be a clicking or snapping feeling.
- Overhead athletes may notice that their throwing distance and velocity decreases.
- However, not everyone who has a SLAP / labral tear will have symptoms. Many people have these injuries and are NOT affected.
Could it be Something Else?
Most people that have sustained a SLAP or Labral tear will have sustained some form of additional damage to their shoulder, either at the time of the injury or preceding it. A number of studies looking at SLAP tears have shown that over 65% of patients had a concomitant / additional shoulder injury.
Commonly occurring additional problems are; AC Joint OA, Weight Lifters Shoulder, Partial Thickness Rotator Cuff Tears, Bankart Tears & Long Head of Biceps Tendonitis.
Find out more about AC Joint OA….
Find out more about Weight Lifters Shoulder….
Find out more about Partial Thickness Cuff Tears….
Find out more about Bankart Tears….
Find out more about Long Head of Biceps Tendonitis….

How do you Diagnose a SLAP Tear?
As with any condition assessment begins with a history and examination of the patient. This may be followed by specific investigations.
History
- Acute SLAP Tear - With traumatic SLAP tears a history of the exact incident, mechanism of injury, subsequent treatment and any further problems is important.
- Chronic SLAP Tear –These injuries tend to occur over time and may not result from a specific incident. A detailed history of the patients sporting and recreational past may be important.

Examination
The clinical examination is the most important element of the diagnostic process.
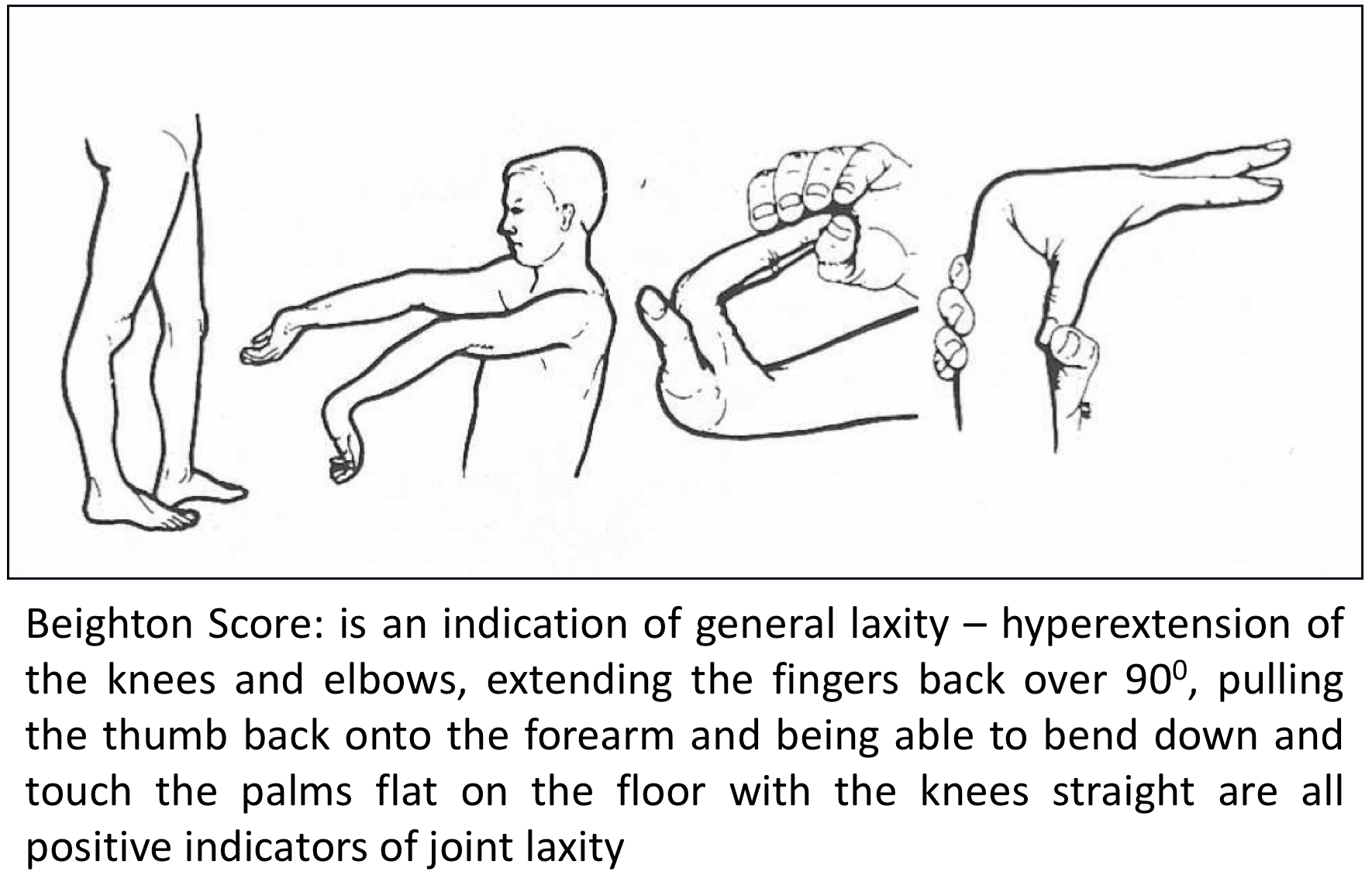
- It is initially important to assess for generalised ligamentous laxity for all patients with SLAP tears. The Bieghton Score is a simple assessment giving a score out of 9 for generalised joint laxity.

- For patients that participate in a specific overhead sport such as tennis, volleyball, javelin etc. it is important to assess their overall core stability
- As with all shoulder problems an initial general examination of both shoulders is undertaken looking for areas of pain, comparing the range of movement and for rotator cuff muscle strength.
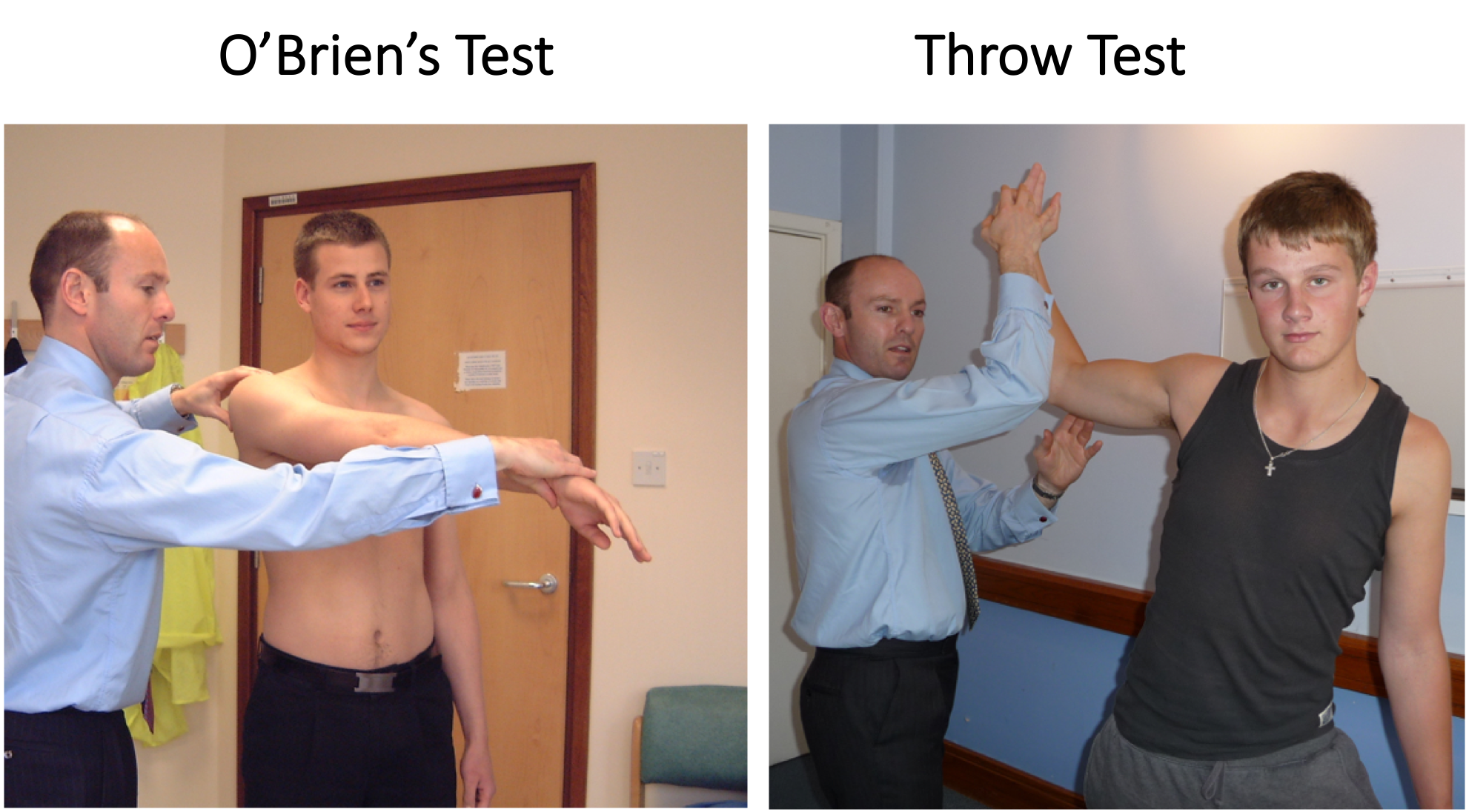
- Special tests are then undertaken specifically to look for SLAP tears and to rule out other conditions. Specialised tests include the O’Briens Test and the Throwing Test.
Investigations
- SLAP & Labral Tears can only be properly visualised on an MRI arthrogram. A plain x-ray, ultrasound scan or CT scan will not be sufficient to make a diagnosis.
- Even with an MRI arthrogram there is a 10 – 20% false negative rate. (the scan does not show a SLAP or Labral tear, but there is one present).
- An MRI arthrogram is also very useful to diagnose any other additional shoulder pathology (AC Joint OA, Partial Thickness Cuff Tear, Bankart Tear).
Treatment of SLAP/Labral Tears
Treatment of someone who has a SLAP or Labral Tear depends on a number of factors. If pain is a predominant problem then medical treatment, rehabilitation and surgery, if these are not successful, is usually required. If the problems tend to only occur when doing a specific activity or sport then there is the additional option of ‘managing’ the problem, either by modifying or adjusting the way someone plays or avoiding the sport.
- Physiotherapy – Physiotherapy assessment and specific Glenohumeral and Scapular stabilising exercises are the main-stay of the initial treatment for a SLAP or Labral tear. By specifically strengthening all of the stabilising structures around the shoulder and increasing the core strength and stability of the scapular stabilizing muscles it is possible to alleviate all of the symptoms related to a SLAP or Labral tear, without requiring surgery.. If pain is a particular feature a short course of NSAIDs prescribed by a Physician can help.

- Analgesia/Pain Relief
- NSAID (Non-Steroidal Anti-Inflammatories) –
- NSAIDs work be reducing the painful inflammatory response, they are useful at all Stages of Frozen Shoulder
- NSAIDs can damage the stomach lining and affect the kidneys. It is important that a patient’s Family Doctor prescribes this medication if it is going to be used for a longer term
- Codeine based Analgesics –
- Codeine based analgesics are pain killers and affect a patient’s perception of pain. As a result, they can have some effect on consciousness depending on their strength
- Codeine based analgesics can lead to constipation if taken for a longer time. Having a high-fibre diet or even taking laxatives might need to be considered
- Nociceptive Analgesics –
- Nociceptive pain killers work on nerve generated pain
- Amitriptyline in lower doses works as a nociceptive pain killer. It has a useful side-effect in that it can make patients drowsy
- in cases of severe pain Amitriptyline can be prescribed at night
- NSAID (Non-Steroidal Anti-Inflammatories) –
- Intraarticular Cortisone Injection –
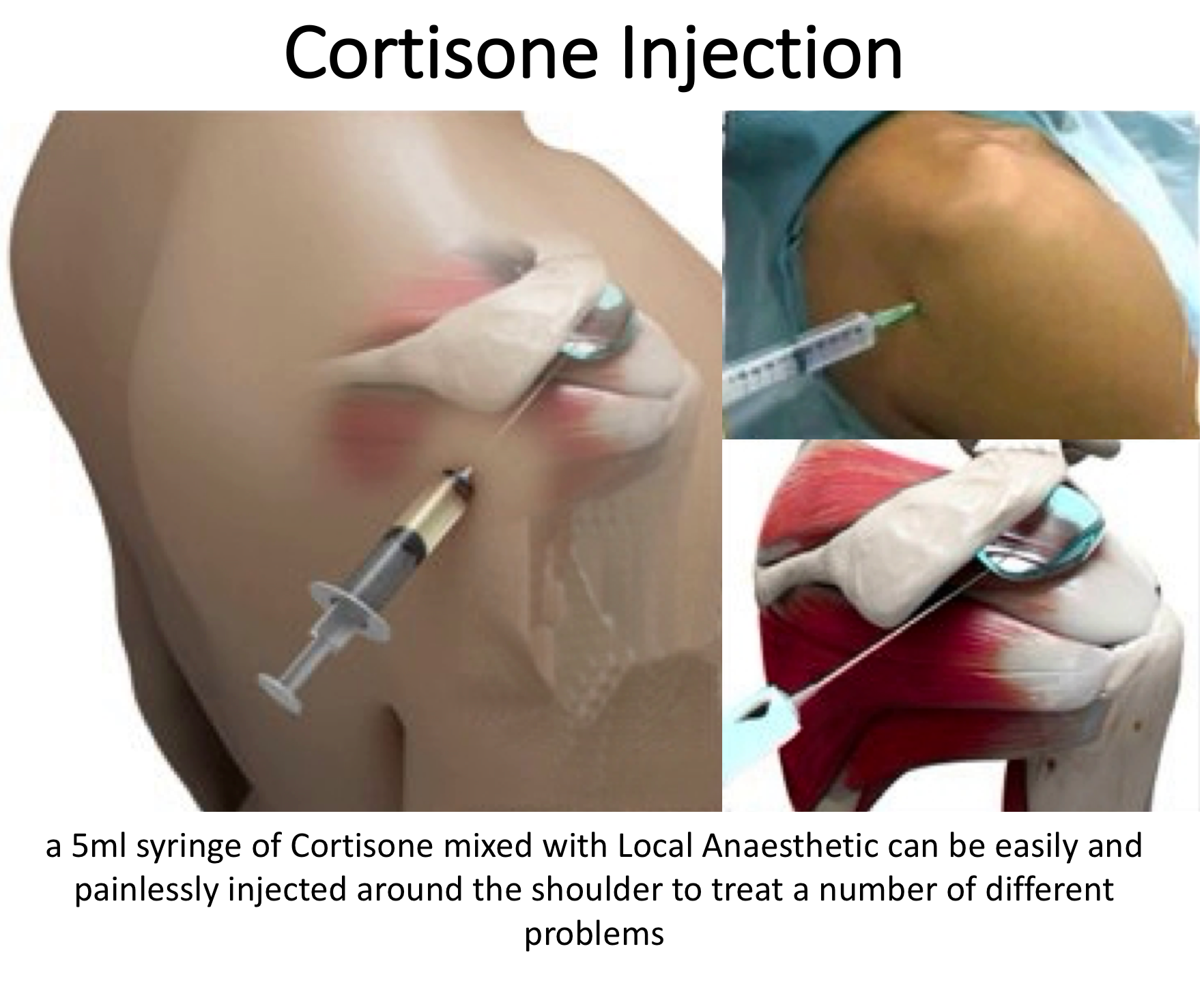
- If someone’s symptoms, particularly pain, have failed to settle, after an adequate course of Physiotherapy, a Intraarticular Cortisone injection can help to settle the symptoms down. Cortisone is a corticosteroid that is naturally produced by the body’s Adrenal Gland. Injectable Cortisone is synthetically produced and has a very powerful ant-inflammatory action. When injected into the Subacromial space it has the potential of settling severe inflammation, allowing the patient to undertake their rehabilitation exercises.
- A Intraarticular Cortisone can be easily administered in the Out-Patient Clinic using Ultrasound guidance. It is a quick and relatively painless procedure. Afterwards patients can continue with their normal day-to-day activities. Occasionally patients can feel a bit of soreness around their shoulder later that day, but this usually passes fairly quickly.
- It often takes several days before someone notices the benefits following a Cortisone injection and sometimes several weeks. The Cortisone works in the background and there is no specific requirement to particularly rest the shoulder or to do extra exercises. The full benefits of a Cortisone injection are usually felt within a month. In some cases, the Cortisone may not give any benefit, this may be an indication of the severity of the Supraspinatus Tendonitis.
- A Cortisone injection only lasts in the body for a few days. Any benefit that someone gets from the Cortisone will be from its acute anti-inflammatory effect allowing the underlying symptoms to settle. If the symptoms do return after a while, it is not because the Cortisone has worn off, but because the inflammation has returned.
- Infections can occur after any type of injection but are extremely rare (1 in 15,000). If someone feels that they are developing an infection within 48 hours of a Cortisone injection they should seek advice from their Family Practitioner.

Surgery for SLAP Tears
- If someone’s shoulder has failed to respond to an adequate rehabilitation program, the only further treatment option to consider, other than persevering with the problem, is surgery. The specific procedure required depends on the Type of SLAP tear and the age of the patient.
- Originally, when SLAP tears were first being noticed on MRI scans and arthroscopic techniques had evolved to fix them, there was an ‘explosion’ in surgical repairs. It seemed that any patient who had a SLAP tear on a scan would undergo surgery.
- However, not every patient who underwent surgery obtained a good result.
- This was extensively investigated and it was realized that, although many patients had SLAP tears, they were not necessarily the cause of the patients symptoms
- It was also noticed that older patients who had a SLAP tear with symptoms didn’t gain as good a recovery as younger patients
- It was found that a Long Head of Biceps Tenodesis gave better results for older patients
Type 2 SLAP – Surgery (under 30 years?)
The aim of surgery for a Type 2 SLAP Tear is to reattach the superior labrum onto the top of the glenoid. This will help to regain shoulder stability and fix the Long Head of Biceps anchor.
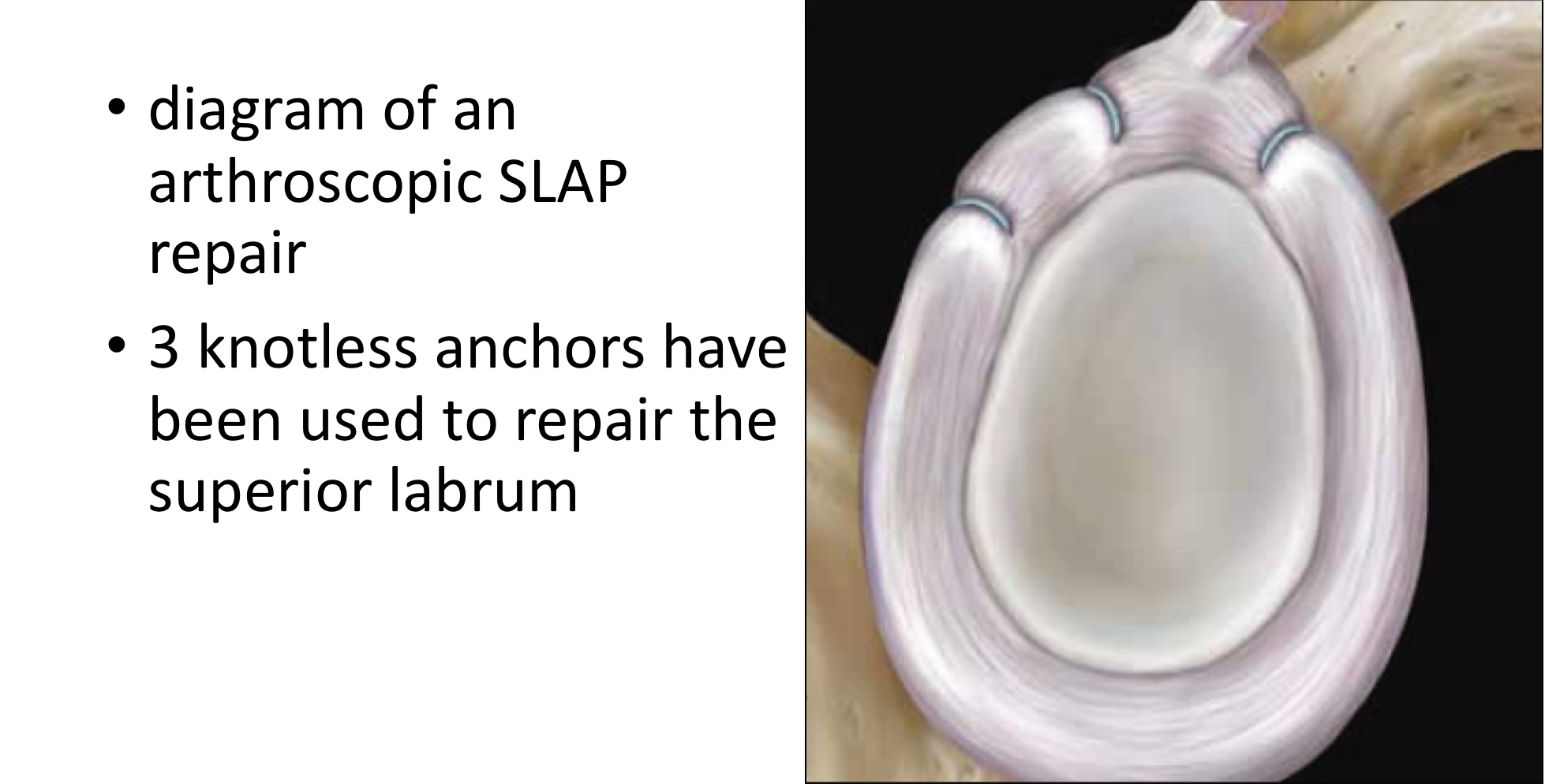
Essentially this involves mobilising and freshening up the torn undersurface of the superior labrum and then re-attaching them on to the top of the Glenoid (Socket), the bone here having also been freshened. The tissue is usually attached to the bone using ‘suture anchors’. These are small implants, made of various materials, that can be inserted, by drill holes, into the bone. Attached to the anchors are sutures that can then be passed through the torn ligaments and capsule and tied down into position. Having re-attached the freshened ligaments and capsule to the freshened bone of the socket they can then heal.
Find out more about suture anchors….

Arthroscopic Type 2 SLAP Repair
A SLAP Repair operation can be only be undertaken as an arthroscopic procedure. The advantages of an arthroscopic procedure are that smaller incisions are used without having to disturb and cut through other structures and it is possible to more accurately assess the damage to the shoulder and quality of repair.
There are a number of different variations to the technique and different implants that can be used. I have evolved my technique over the past 15 years, taking advantage of new implants and equipment, and have obtained consistently good results, with which I am happy. My routine Type 2 SLAP Repair is described below,
Watch a video of an arthroscopic SLAP Repair….
Find out more about Arthroscopic Shoulder Surgery….
Procedure
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
- Prophylactic iv antibiotics are given
- A posterior, an anterior and a superior lateral portal are used for joint access
- The joint is initially assessed to confirm the presence of a Type 2 SLAP tear and for any other pathology
- The torn labrum is then fully mobilised and the tissues freshened
- The Superior Glenoid edge is then prepared and freshened
- 1 - 3 Osteoraptor or Pushlok bio-composite anchors are inserted into the superior glenoid (as required) and the labrum reattached
- The repair is assessed and the wounds closed

After the Surgery
Post-Operative Care
Following an Arthroscopic SLAP Repair the patient may be able to go home that day or may need to stay in the Hospital overnight, depending on circumstances. I would see the patient after the surgery to discuss how the procedure has gone and arrange for further Follow-Up. The patient will be seen by the In-Patient Physiotherapy team who will instruct them on how to take the sling on and off and the ‘safe zones’ of movement. Further physiotherapy will then be organised from the 3 week mark onwards.
Find out more about Physiotherapy following Shoulder Surgery….
I would usually review patients in the clinic 1 month, 3 months and 6 months after their procedure to assess their progress and recovery.

Period of Sling Immobilisation & Rehabilitation Protocol
After an arthroscopic SLAP Repair the patient’s arm needs to be in a sling for 2 - 3 weeks. It is initially important to ‘protect’ the repair from any significant load as it begins to heal whilst, at the same time, it is preferable to not allow the shoulder to get too stiff. The physiotherapists will instruct the patient on the ‘safe zones’ of movement out of their sling over this period.
My standard rehabilitation protocol is outlined below. The information and time to recovery are a general estimation and may vary from person to person.
|
Post op |
|
| Immediate |
|
| Day 1-3
Weeks |
|
| 3-6 Weeks |
|
| 6 Weeks + |
|
| Milestones | |
| Week 6 | Active range of movement at least 75% of normal |
| Week 12 | Full ROM, with minor loss of combined abduction and external rotation |
|
Return to Functional Activities |
|
| Driving |
|
| Swimming |
|
| Golf |
|
| Contact &ThrowingSport |
|
| Lifting |
|
| Work |
|
Success of Surgery, Risks & Complications
Success following an Arthroscopic Bankart Repair has to be assessed slightly differently from other procedures. Rather than being able to measure how much better the shoulder is after the operation we are waiting for a further dislocation NOT to happen. By convention, for a stabilisation procedure to be considered successful, the patient needs to have had no episodes of instability for at least 2 years after their operation.
For a standard Arthroscopic Bankart Repair >90% of patients’ shoulders will be stable 2 years after their surgery. For patients returning to contact sports this figure is decreased to > 80%.
There are always risks and complications associated with any operation.
- Anaesthetic - The risks of having a General Anaesthetic and an Interscalaene Nerve Block are very low, but will always need to be assessed on an individual basis by an Anaesthetist. Suffice it to say, that whilst a Shoulder Operation can in no way be considered a ‘life-saving’ procedure, an Anaesthetist would not consider undertaking an anaesthetic if they had any concerns that an undue risk was being taken.
- Recurrence – The 2- year re-dislocation rate <10% (for Contact Athletes <20%)
- Infection – Infection following arthroscopic surgery is rare < 0.2%
- Neurovascular Injury – Damage tosignificant neurovascular structures during arthroscopic shoulder surgery is rare < 0.2%
- CRPS Type 1 – A Chronic Pain Syndrome following arthroscopic shoulder surgery is rare < 0.2%
Outcome Measures
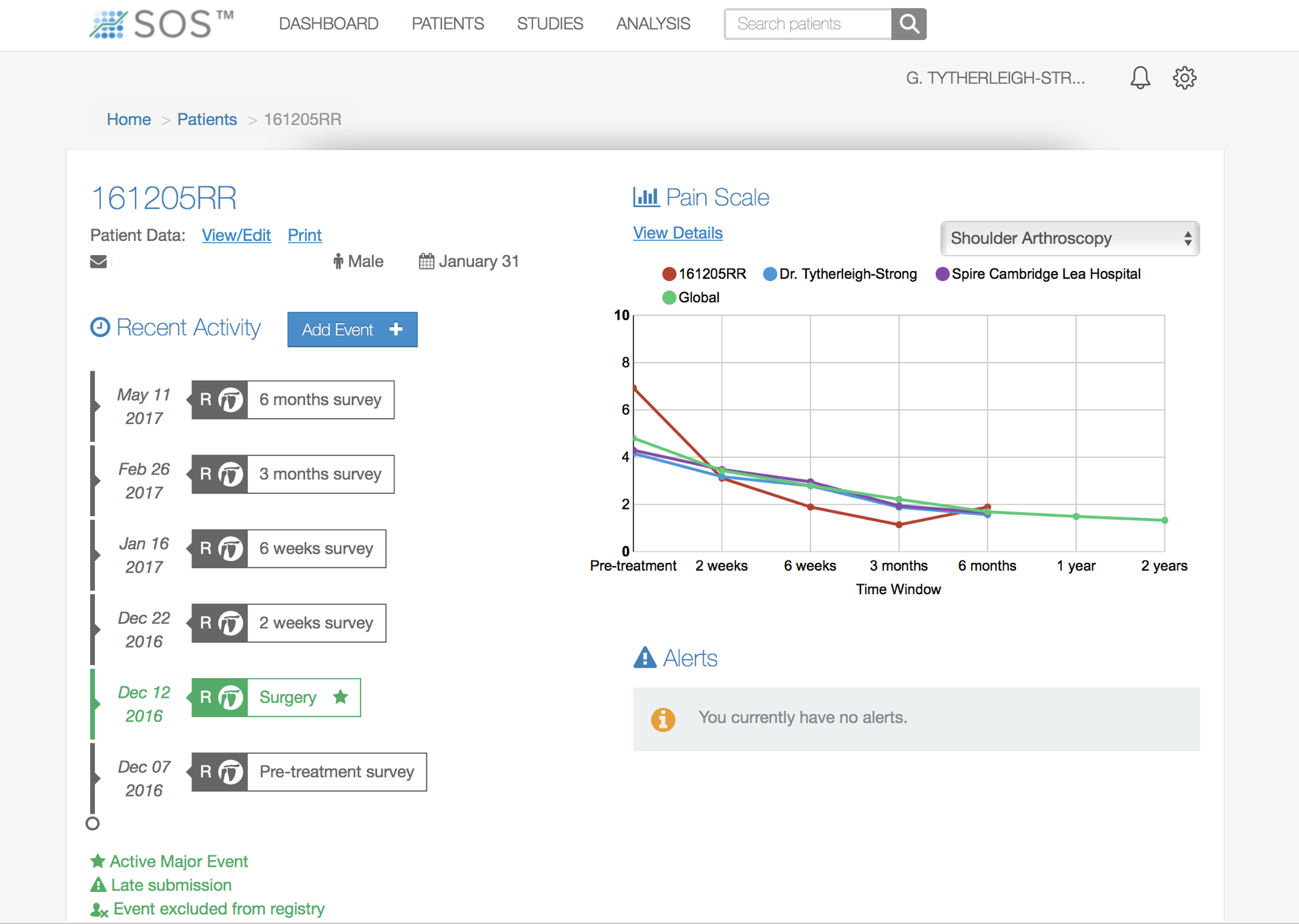
Assessing patient outcomes following surgery, using validated scoring systems, is a very important and useful exercise.
Find out more about Outcome Measures and the SOS system …..
Type 4 SLAP - Surgery (Type 2 SLAP Tears in patients over 30 years)
The main cause for symptoms with a Type 4 SLAP tear are due to the damage to the insertion of the Long Head of Biceps, rather than from the damage to the Labrum. Accordingly, the most appropriate surgery to address this problem is to undertake a Long Head of Biceps Tenodesis.
I prefer to undertake a Sub-Pectoral Long Head of Biceps Tenodesis for younger patients, particularly if there are involved in sport.
Arthroscopic Long Head of Biceps Tenodesis
An LHB Tenodesis involves detaching the LHB at its origin in the shoulder, as in a Tenotomy, and then re-attaching the tendon at some point on the humerus. Following a Tenodesis the LHB continues to work as a biceps tendon.
An Arthroscopic LHB Tenodesis can usually be done as a Day Case procedure. The patient’s shoulder does not usually need to be immobilized for anytime afterwards. The surgery aims to detach the LHB tendon from its insertion in the shoulder and then to re-attach it at the bottom of the bicipital groove, just below the insertion of Pectoralis Major. Recovery is usually fairly rapid and within 4 - 6 weeks most patients have gained the full benefits of the procedure. It has a high success rate with around 95% of patients being happy with the result 3 - 6 months after their operation. My routine LHB Tenodesis Procedures all commence with an Arthroscopic Tenotomy and are described below.
Find out more about Arthroscopic Surgery….
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
- A posterior and a single anterior portal are used to view the Gleno-Humeral Joint (Shoulder Joint)
- The Glenohumeral Joint is initially assessed to look for any other problems that might be associated with an LHB tenodonitis, in particular, the superior labrum
- The LHB is then probed and the extent of the Type 4 split assessed.
- Using an arthroscopioc punch, shaver or radiofrequency probe the LHB tendon is then divided at its base where it joins the glenoid labrum. The tendon then usually retracts out of the joint
- The top of the labrum is then debrided to a neat rim.
Sub-Pectoral Tenodesis –
- This part of the procedure is undertaken as an open operation
- A 3cm longitudinal incision is made in the crease of the axilla and, retracting the Deltoid superiorly, dissection taken down onto the shaft of the humerus
- The LHB tendon is identified, and having been cut proximally, pulled out of the wound
- A whip-stitch is then sutured from the musculotendinous junction of the biceps about 1.5cm up the tendon. The rest of the redundant tendon is then cut and discarded
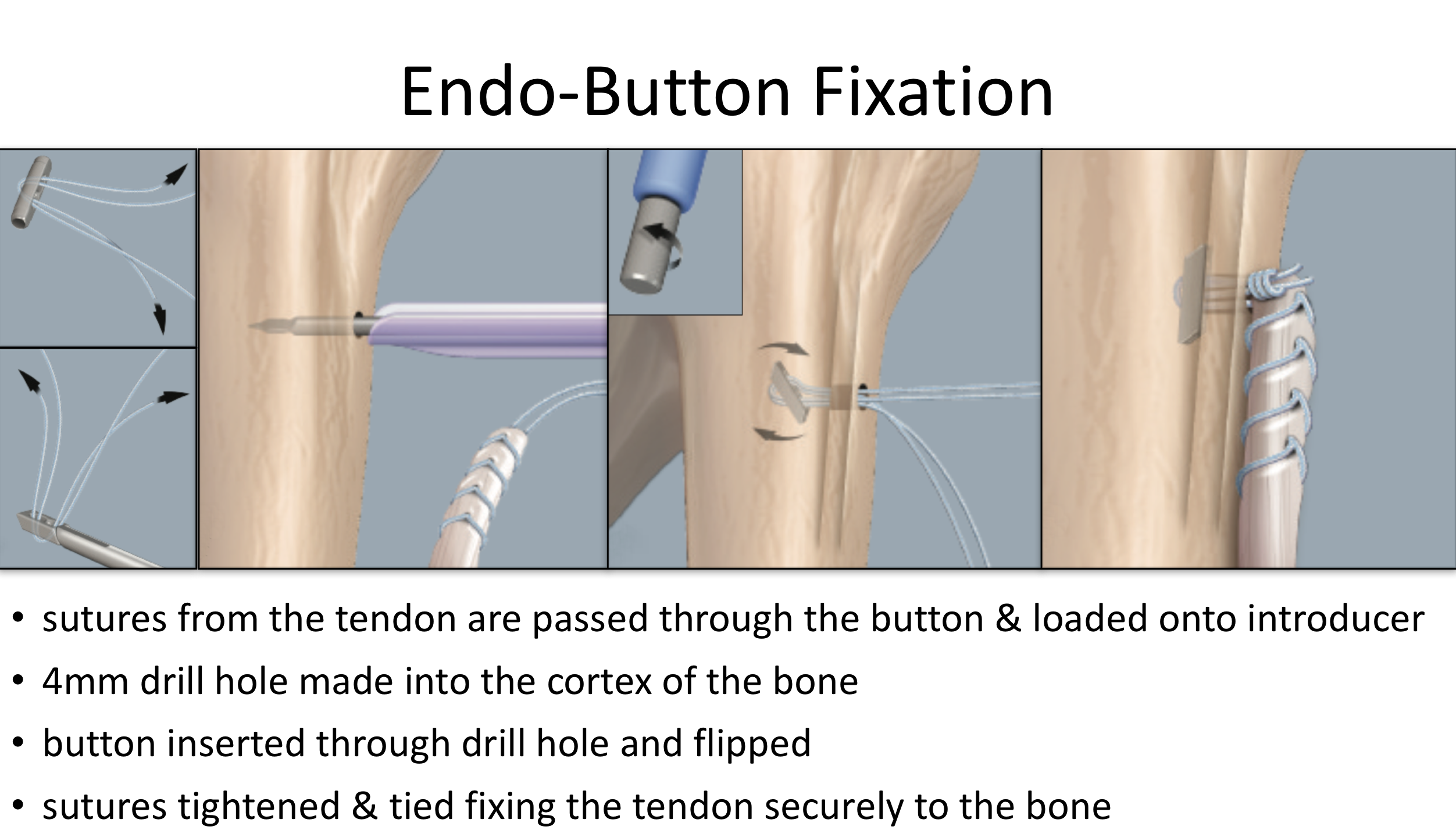
- The suture ends are then passed through the Endo-Button which is mounted onto an introducer
- The shaft of the humerus is then exposed and a 4mm hole drilled through the cortex just below the pectoralis major
- The loaded Endo-Button is then inserted through the drill hole in the humeral shaft. The button is then ‘flipped’ within the medullary canal of the bone and the sutures tightened through the button. This brings the end of the tendon onto the bone and the construct is tightened to an appropriate tension
After the Surgery
Post-Operative Care
Following an LHB tnodesis the patient is usually able to go home on the same day as their surgery. However, this may vary if any additional procedures have also been undertaken at the same time. I would see the patient after the surgery to discuss how the procedure has gone and arrange for further Follow-Up. The patient will be seen by the In-Patient Physiotherapy team, who will instruct them on the initial Rehabilitation Protocol for their shoulder. Further Out-Patient physiotherapy will then be organised.
Find out more about Physiotherapy following LHB Surgery….
I would usually review patients in the clinic 1 month and 3 months after their procedure to assess their progress and recovery.
Rehabilitation Protocol
Immediately after the surgery, when the patient has woken up from their general anaesthetic, their shoulder and arm will be numb from the interscalaene nerve block. This will usually last for 18 – 24 hours after the surgery. For this period, we advise patients to keep their arm in a sling, purely for protection. After the nerve block has worn off the arm can begin to be taken out of the sling. I encourage patients to wean themselves from using the sling as quickly as possible, within the limits of discomfort.
My standard rehabilitation protocol is outlined below. The information and time to recovery are a general estimation and may vary from person to person. If any additional procedure has been undertaken at the same time, the rehabilitation protocol for that procedure would usually supersede that of the Tenodesis.
|
Post op |
|
| Immediate |
|
| Day 1-3
Weeks |
|
| 3-6 Weeks |
|
| 3 Months |
|
| Milestones | |
| Week 2 - 3 | Full passive range of movement |
| Week 6 | Full active range of movement, good scapular control |
|
Return to Functional Activities |
|
| Driving |
|
| Swimming |
|
| Golf |
|
| Racquet Sports/Repeated |
|
| Weight Training Overhead Activities |
|
| Lifting |
|
| Work |
|
Success of Surgery, Risks & Complications
An LHB Tenodesis is usually a very successful procedure and most people notice a significant improvement in their pain within 4 weeks. Very occasionally people can experience an ache or cramping pain just above the location of the tenodesis, this may correspond to a residual tendonitis within the remaining tendon. This does not usually occur with a Sub-Pectoral Tenodesis as all of the residual LHB tendon has been excised. This pain usually settles with time and can be aided by an ultrasound guide cortisone injection.
There are always risks and complications associated with any operation.
- Anaesthetic - The risks of having a General Anaesthetic and an Interscalaene Nerve Block are very low, but will always need to be assessed on an individual basis by an Anaesthetist. Suffice it to say, that whilst a Shoulder Operation can in no way be considered a ‘life-saving’ procedure, an Anaesthetist would not consider undertaking an anaesthetic if they had any concerns that an undue risk was being taken.
- Infection – Infection following arthroscopic surgery is rare < 0.2%
- Neurovascular Injury – Damage tosignificant neurovascular structures during arthroscopic shoulder surgery is rare < 0.2%
- CRPS Type 1 – A Chronic Pain Syndrome following arthroscopic shoulder surgery is rare < 0.2%
Outcome Measures
Assessing patient outcomes following surgery, using validated scoring systems, is a very important and useful exercise.
Find out more about Outcome Measures and the SOS system …..