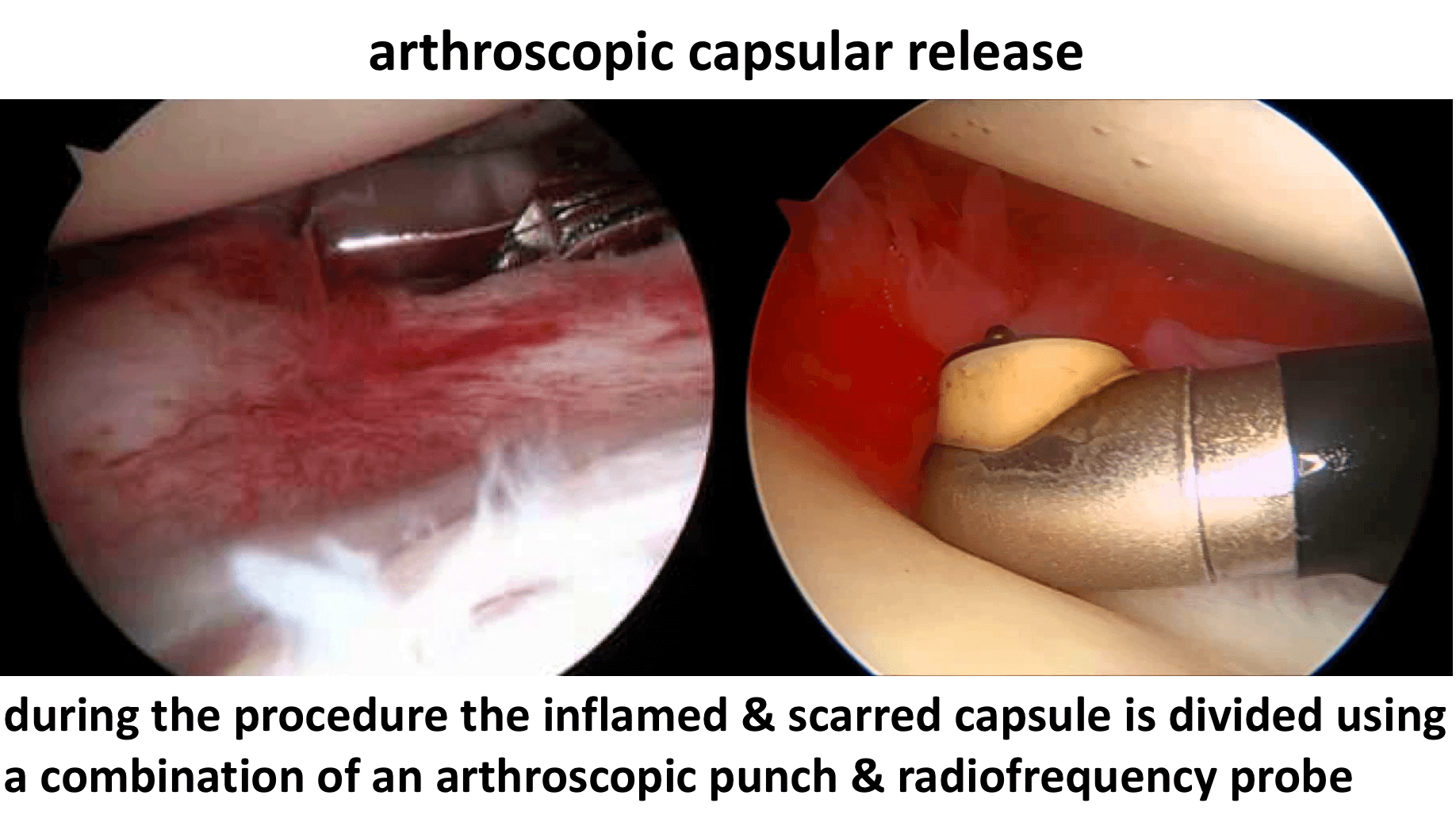







Arthroscopic Capsular Release
An Arthroscopic Capsular Release is usually done as an In-Patient procedure and the patient’s shoulder does not need to be immobilized for anytime afterwards. The surgery aims to circumferentially release the scar tissue from around the whole shoulder and tidy up the rest of the joint. At the same time the rest of the shoulder can be assessed and an Arthroscopic Subacromial Decompression undertaken. After the surgery it is essential to keep the shoulder as mobile as possible to prevent the scar tissue reforming. The procedure is undertaken using a general anaesthetic, an interscaelane nerve block and an additional pain pump. The pain pump contains 250ml of local anaesthetic and is connected to the shoulder through a small 2mm diameter tube. The pump delivers a constant flow of local anaesthetic into the shoulder for the next few days, keeping the shoulder comfortable. The next day the Physiotherapists take the patient through several intensive sessions of physiotherapy to help maintain the recovered range of motion and to regain strength. My routine Arthroscopic Capsular Release Procedure is described below,

Watch a video of an Arthroscopic Capsular Release….
Find out more about Arthroscopic Shoulder Surgery…
- The patient is anaesthetised with a general anaesthetic and interscaelane nerve block
Find out more about having an anaesthetic….
Find out more about an Interscalene Nerve Block….
- A posterior and a single lateral portal are used to view the Gleno-Humeral Joint (Shoulder Joint) and Subacromial spaces
- The Glenohumeral Joint is initially assessed to assess for the extent of the capsular contracture and any other associated problems, in particular, the Rotator Cuff and the Long Head of Biceps
- An anterior portal is then created and an extensive capsular release undertaken using a combination of an arthroscopic punch, shaver and radiofrequency probe (Fig 7)
- The Subacromial Space is then entered and the undersurface of the Acromion identified.
- A lateral portal is then created
- Using a combination of a powered shaver and radiofrequency probe the coracoacromial ligament is released, revealing the Subacromial Spur.
- A powered burr is then used to resect about 5mm of bone from the undersurface of the acromion
- The Decompression is then assessed to check that sufficient bone has been resected
- The tube for the Subacromial Pain Pump is then inserted
- If any significant damage is found to the Rotator Cuff this will be then also be repaired
- The Subacromial Space is then washed out and the wounds closed with sub-cuticular sutures
Find out more about having an operation…